

C3 glomerulopathies: dense deposit disease and C3 glomerulonephritis
- PMID: 38076230
- PMCID: PMC10704907
- DOI: 10.3389/fmed.2023.1289812
C3 glomerulopathies: dense deposit disease and C3 glomerulonephritis
Abstract
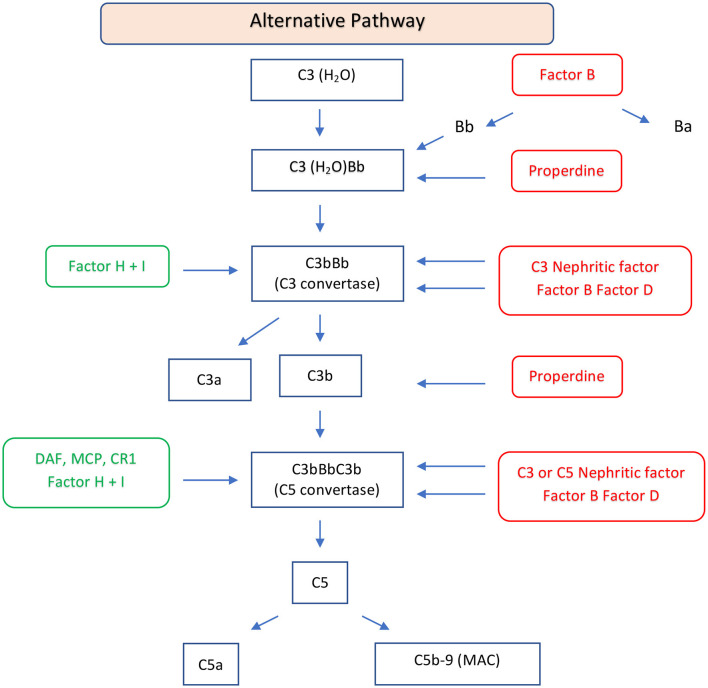
Dense deposit disease (DDD) and C3 glomerulonephritis (C3GN) are types of membranoproliferative glomerulonephritis classified as C3 glomerulopathies. These conditions are characterized by an increased number of intraglomerular cells and diffuse thickening of the glomerular capillary walls, along with the deposition of C3 and minimal or absent immunoglobulin deposits. The underlying cause of both DDD and C3Gn is an abnormal activation of the alternative complement pathway, which can result from acquired or genetic alteration. In acquired forms of DDD and C3GN, the dysregulation of the alternative pathway is commonly induced by the presence of C3 nephritic factors (C3NeFs), which are autoantibodies that stabilize C3 convertase. Both DDD and C3GN can affect individuals of any age, but DDD is primarily diagnosed in children, whereas C3GN tends to be diagnosed at a significantly higher age. The presenting features of these diseases are variable and may include proteinuria, hematuria, hypertension, or kidney failure. A common finding in these diseases is low serum C3 levels with normal serum C4 levels. Chronic deterioration of renal function is commonly observed in DDD and C3GN, often leading to end-stage renal disease (ESRD), especially in DDD. Kidney transplantation outcomes in patients with these conditions are characterized by histological recurrence, which may contribute to higher rates of allograft failure.
Keywords: C3 glomerulonephritis; C3 glomerulopathies; alternative complement pathway; dense deposit disease; membra-noproliferative glomerulonephritis.
Copyright © 2023 Ponticelli, Calatroni and Moroni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Servais A, Frémeaux-Bacchi V, Lequintrec M, Salomon R, Blouin J, Knebelmann B, et al. . Primary glomerulonephritis with isolated C3 deposits: a new entity which shares common genetic risk factors with haemolytic uraemic syndrome. J Med Genet. (2007) 44:193–9. 10.1136/jmg.2006.045328 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous