

Pregnancy after kidney transplantation: 40 years single-center experience
- PMID: 38078833
- PMCID: PMC11210546
- DOI: 10.1590/2175-8239-JBN-2023-0061en
Pregnancy after kidney transplantation: 40 years single-center experience
Abstract
Background: Kidney transplantation (KT) improves quality of life, including fertility recovery.
Objective: to describe outcomes of post-KT pregnancy and long-term patient and graft survival compared to a matched control group of female KT recipients who did not conceive.
Methods: retrospective single-center case-control study with female KT recipients from 1977 to 2016, followed-up until 2019.
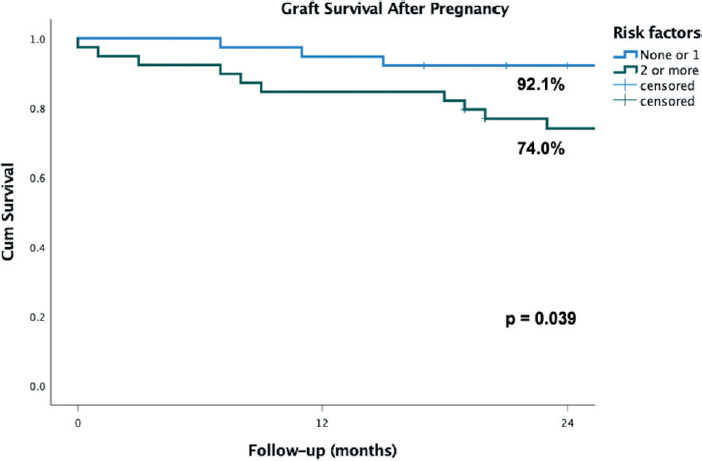
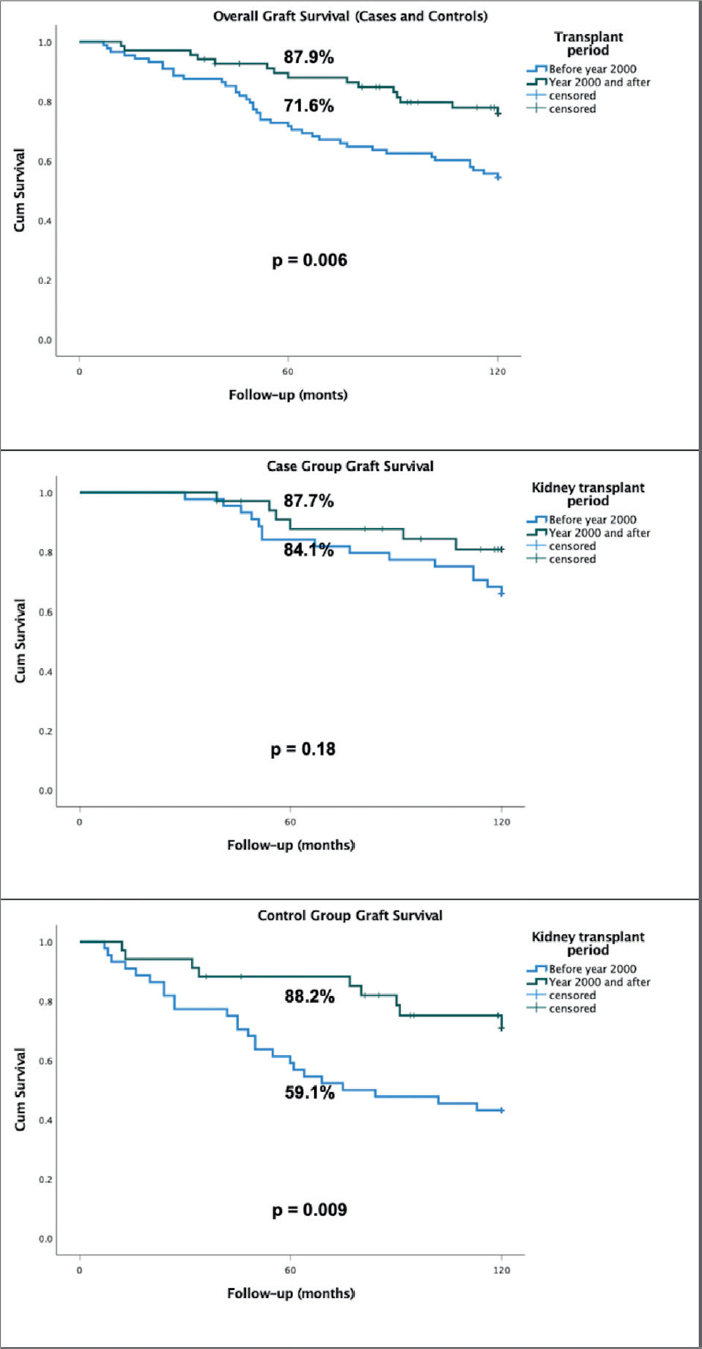
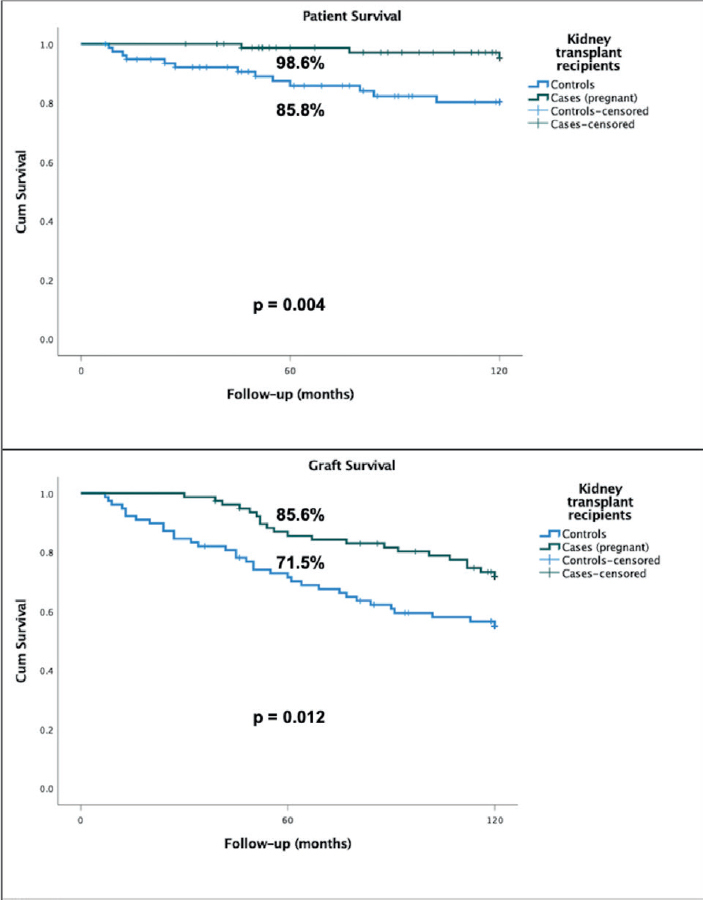
Results: there were 1,253 female KT patients of childbearing age in the study period: 78 (6.2%) pregnant women (cases), with a total of 97 gestations. The median time from KT to conception was 53.0 (21.5 - 91.0) months. Abortion rate was 41% (spontaneous 21.6%, therapeutic 19.6%), preterm delivery, 32%, and at term delivery, 24%. Pre-eclampsia (PE) occurred in 42% of pregnancies that reached at least 20 weeks. The presence of 2 or more risk factors for poor pregnancy outcomes was significantly associated with abortions [OR 3.33 (95%CI 1.43 - 7.75), p = 0.007] and with kidney graft loss in 2 years. The matched control group of 78 female KT patients was comparable on baseline creatinine [1.2 (1.0 - 1.5) mg/dL in both groups, p = 0.95] and urine protein-to-creatinine ratio (UPCR) [0.27 (0.15 - 0.44) vs. 0.24 (0.02 - 0.30), p = 0.06]. Graft survival was higher in cases than in controls in 5 years (85.6% vs 71.5%, p = 0.012) and 10 years (71.9% vs 55.0%, p = 0.012) of follow-up.
Conclusion: pregnancy can be successful after KT, but there are high rates of abortions and preterm deliveries. Pre-conception counseling is necessary, and should include ethical aspects.
Histórico:: Transplante renal (TR) melhora qualidade de vida, incluindo recuperação da fertilidade.
Objetivo:: descrever desfechos gestacionais pós-TR e sobrevida de longo prazo da paciente e do enxerto renal comparada a um grupo controle pareado de receptoras de TR que não conceberam.
Métodos:: estudo retrospectivo caso-controle com receptoras de TR de 1977 a 2016, acompanhadas até 2019.
Resultados:: foram identificadas 1.253 receptoras de TR em idade fértil no período do estudo: 78 (6,2%) gestantes (casos), total de 97 gestações. Tempo mediano entre TR até concepção foi 53,0 (21,5 – 91,0) meses. Taxa de aborto foi 41% (espontâneo 21,6%, terapêutico 19,6%), parto prematuro, 32%, e a termo, 24%. Pré-eclâmpsia (PE) ocorreu em 42% das gestações que alcançaram pelo menos 20 semanas. Presença de 2 ou mais fatores de risco para desfechos gestacionais desfavoráveis foi significativamente associada a abortos [OR 3,33 (IC95% 1,43 – 7,75), p = 0,007] e perda de enxerto renal em 2 anos. O grupo controle de 78 mulheres com TR foi comparável na creatinina basal [1,2 (1,0 – 1,5) mg/dL nos dois grupos, p = 0,95] e na relação proteína/creatinina urinária (RPCU) [0,27 (0,15 – 0,44) vs. 0,24 (0,02 – 0,30), p = 0,06]. Sobrevida do enxerto foi maior nos casos que nos controles em 5 anos (85,6% vs. 71,5%, p = 0,012) e 10 anos (71,9% vs. 55,0%, p = 0,012) de acompanhamento.
Conclusão:: a gestação pode ser bem-sucedida após TR, mas existem altas taxas de abortos e partos prematuros. Aconselhamento pré-concepção é necessário e deve incluir aspectos éticos.
Conflict of interest statement
Figures
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LYC, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341((23)):1725–30. doi: 10.1056/NEJM199912023412303. - DOI - PubMed
-
- Registro Brasileiro de Transplantes [cited 2023 Oct 16];Dimensionamento dos Transplantes no Brasil e em cada Estado. 2021 :2014–2021. Available from: https://site.abto.org.br/conteudo/rbt/
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
