

Imaging for the assessment of the arrhythmogenic potential of mitral valve prolapse
- PMID: 38078997
- PMCID: PMC11164824
- DOI: 10.1007/s00330-023-10413-9
Imaging for the assessment of the arrhythmogenic potential of mitral valve prolapse
Abstract
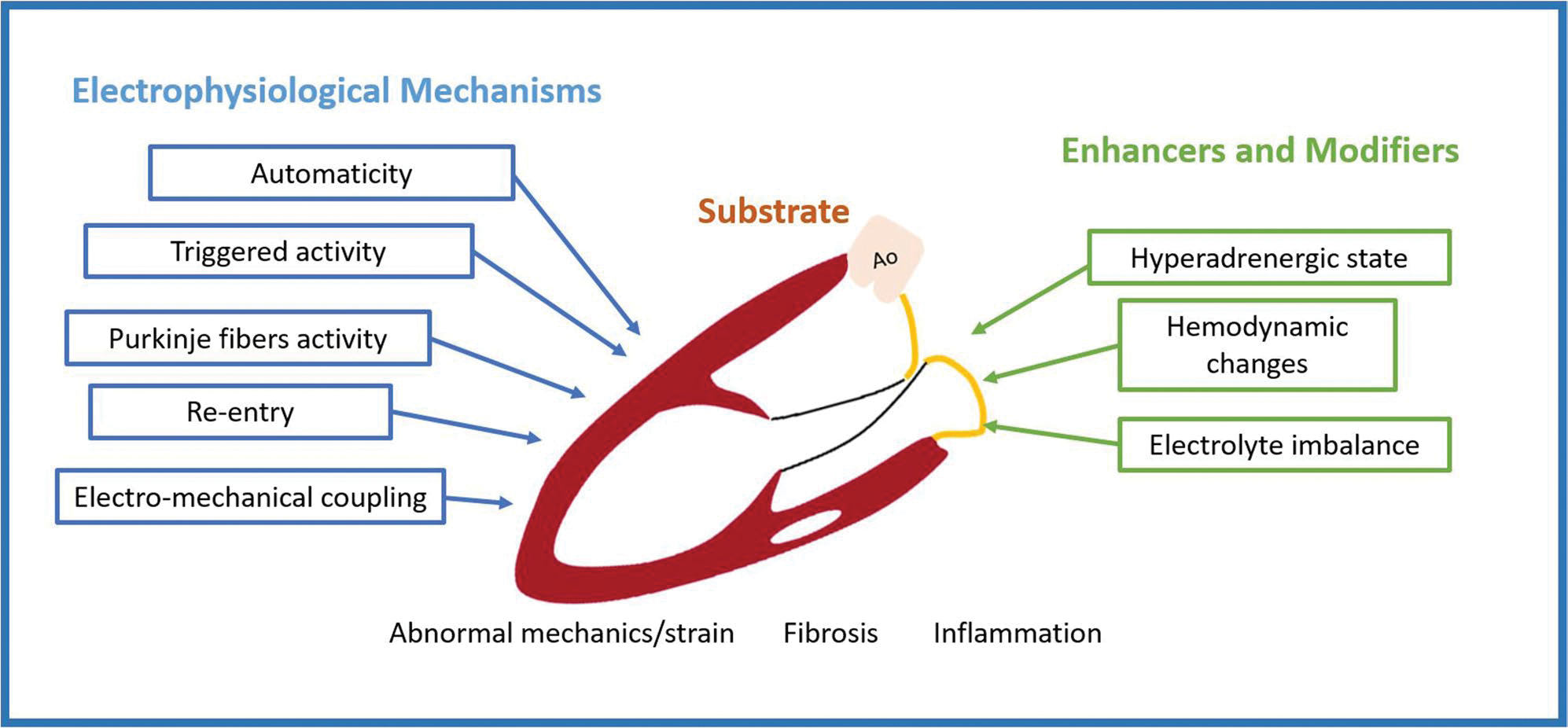
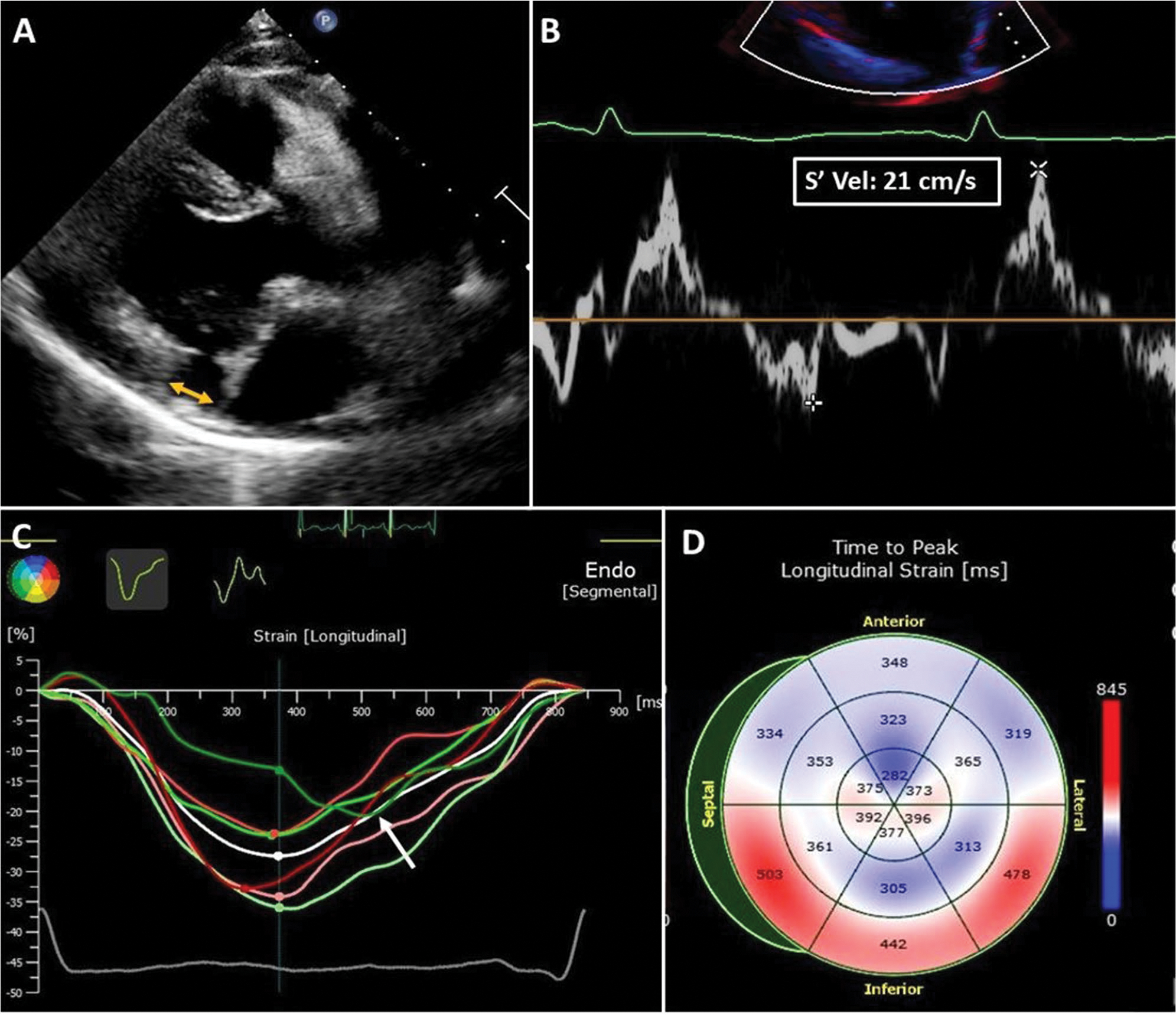
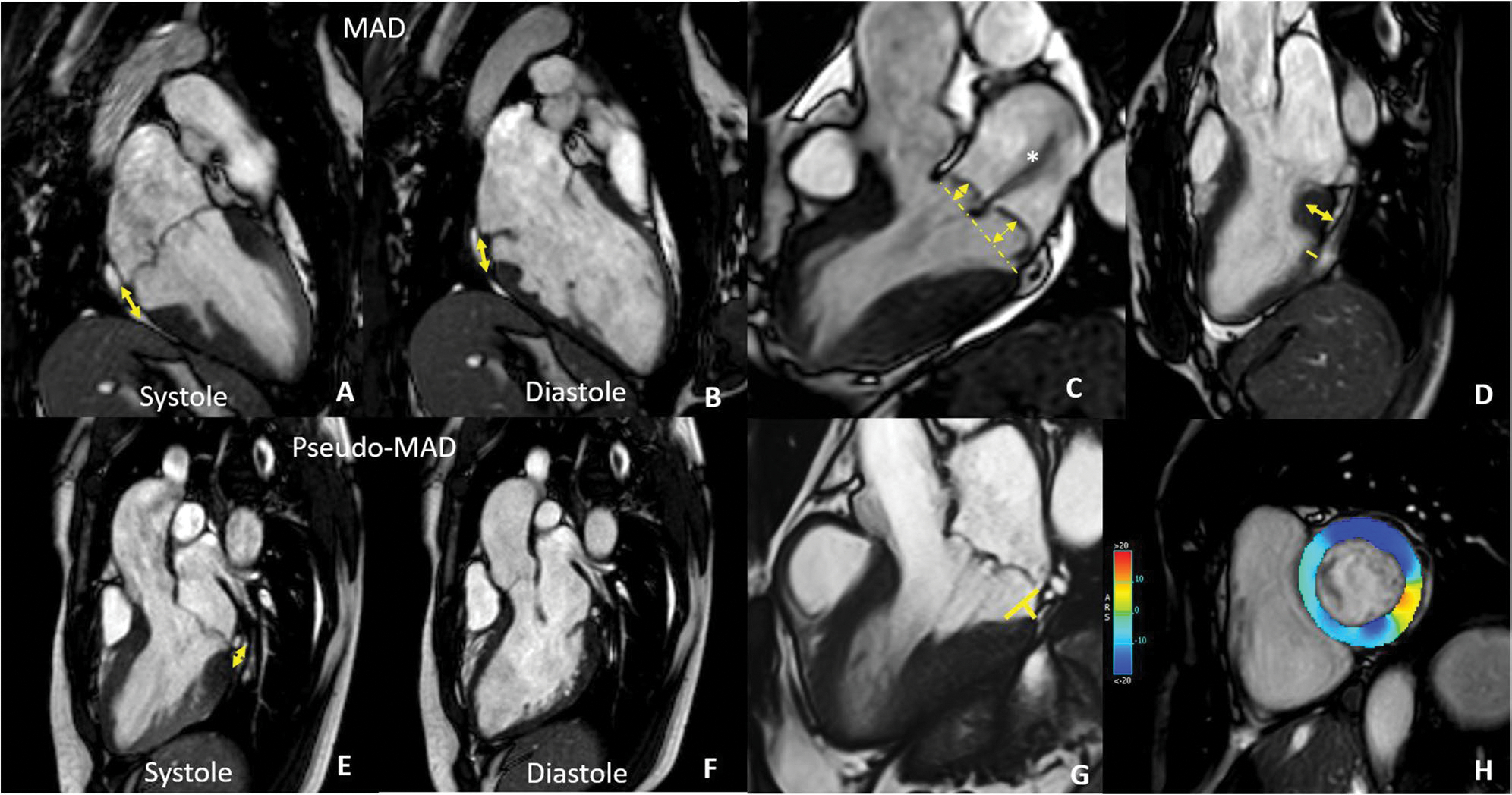
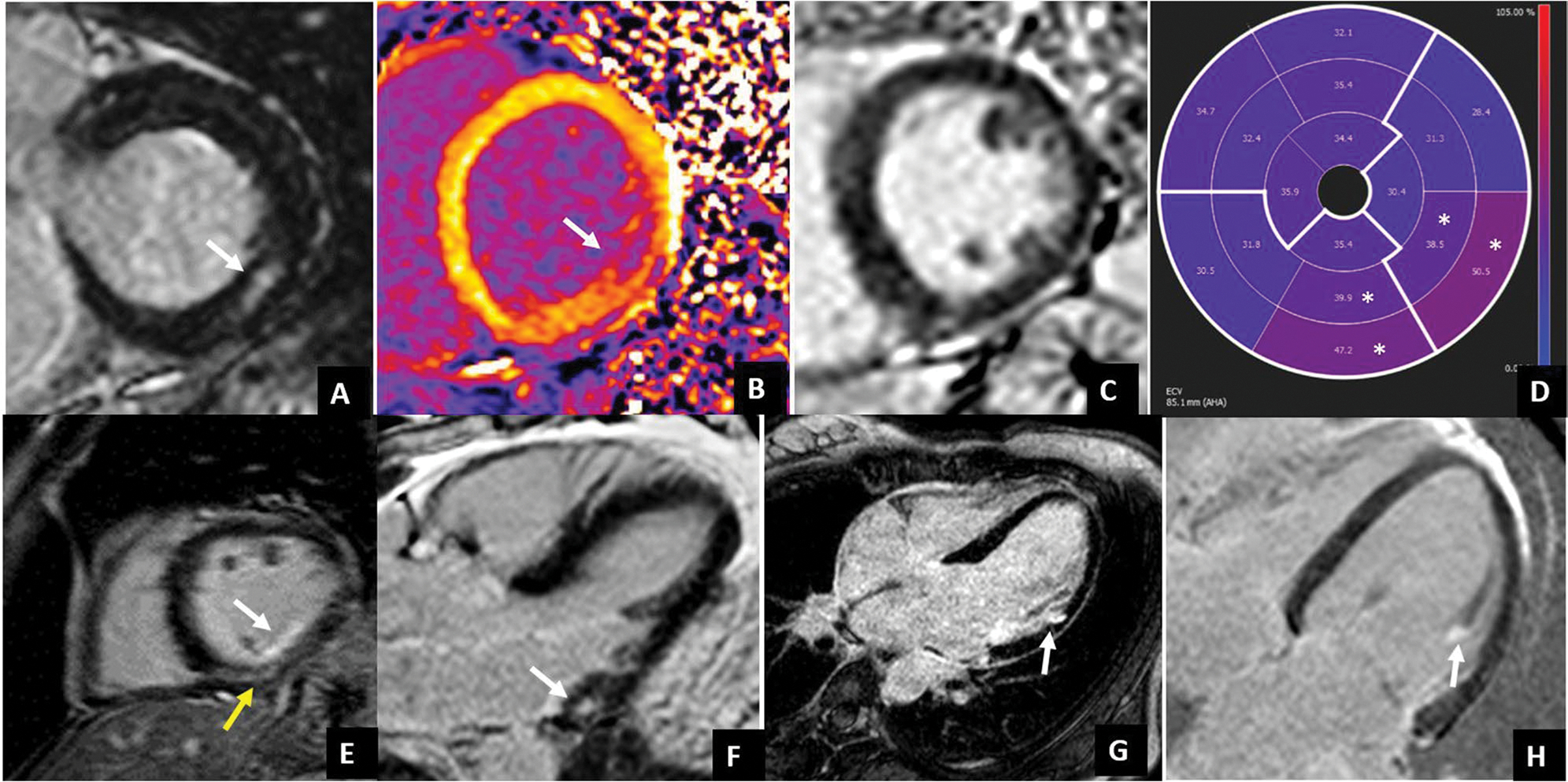
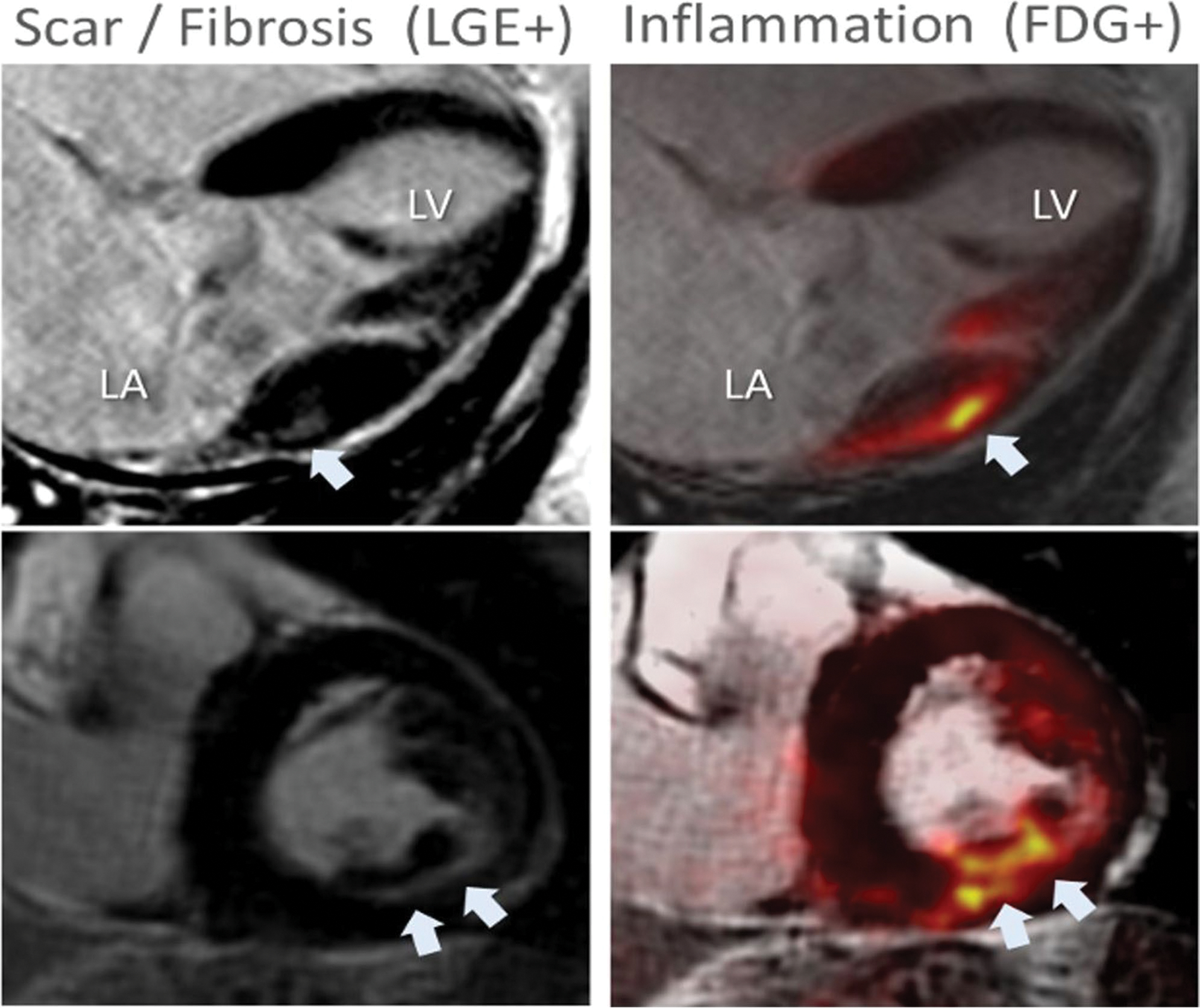
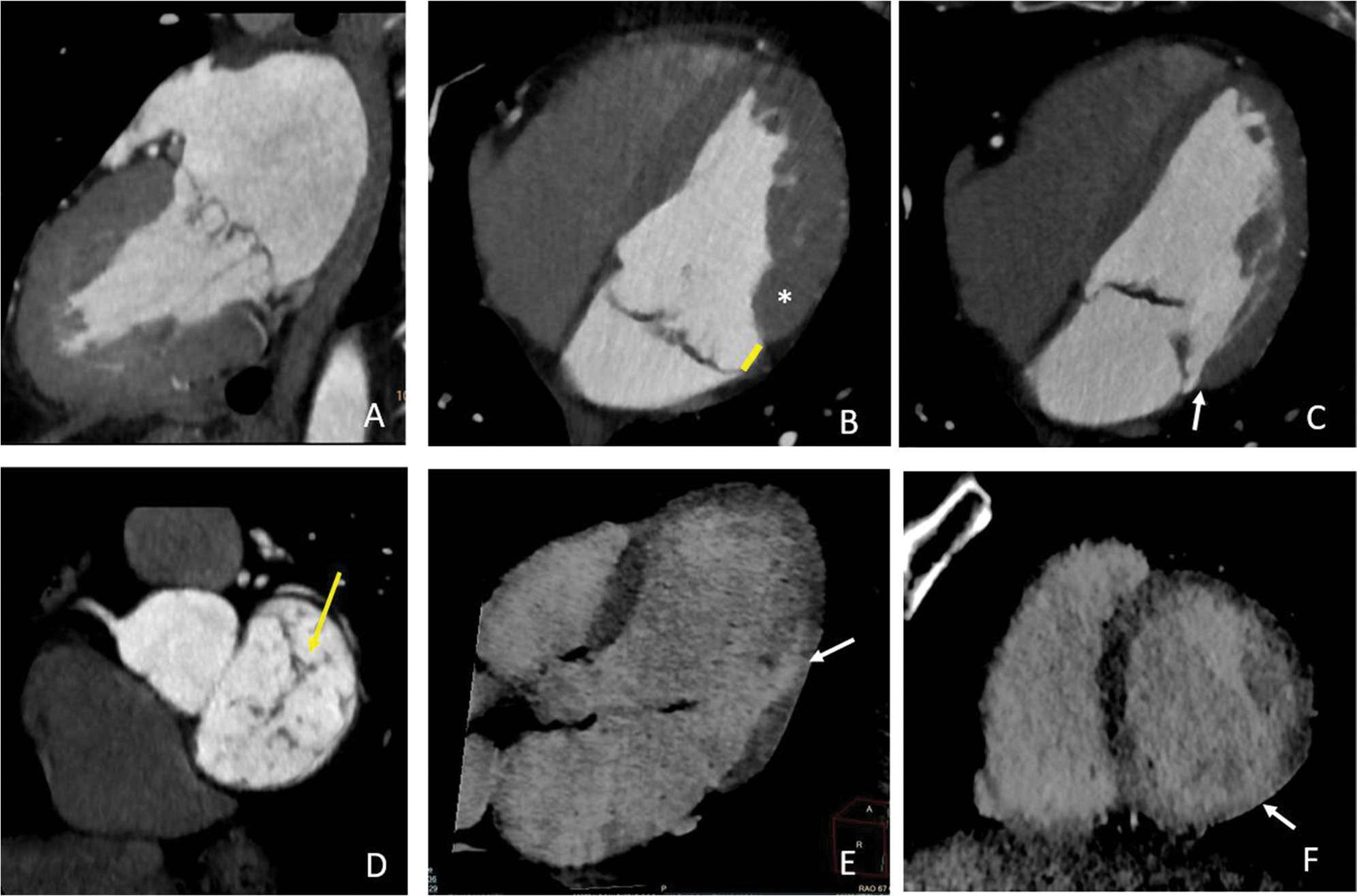
Mitral valve prolapse (MVP) is the most common valve disease in the western world and recently emerged as a possible substrate for sudden cardiac death (SCD). It is estimated an annual risk of sudden cardiac death of 0.2 to 1.9% mostly caused by complex ventricular arrhythmias (VA). Several mechanisms have been recognized as potentially responsible for arrhythmia onset in MVP, resulting from the combination of morpho-functional abnormality of the mitral valve, structural substrates (regional myocardial hypertrophy, fibrosis, Purkinje fibers activity, inflammation), and mechanical stretch. Echocardiography plays a central role in MVP diagnosis and assessment of severity of regurgitation. Several abnormalities detectable by echocardiography can be prognostic for the occurrence of VA, from morphological alteration including leaflet redundancy and thickness, mitral annular dilatation, and mitral annulus disjunction (MAD), to motion abnormalities detectable with "Pickelhaube" sign. Additionally, speckle-tracking echocardiography may identify MVP patients at higher risk for VA by detection of increased mechanical dispersion. On the other hand, cardiac magnetic resonance (CMR) has the capability to provide a comprehensive risk stratification combining the identification of morphological and motion alteration with the detection of myocardial replacement and interstitial fibrosis, making CMR an ideal method for arrhythmia risk stratification in patients with MVP. Finally, recent studies have suggested a potential role in risk stratification of new techniques such as hybrid PET-MR and late contrast enhancement CT. The purpose of this review is to provide an overview of the mitral valve prolapse syndrome with a focus on the role of imaging in arrhythmic risk stratification. CLINICAL RELEVANCE STATEMENT: Mitral valve prolapse is the most frequent valve condition potentially associated with arrhythmias. Imaging has a central role in the identification of anatomical, functional, mechanical, and structural alterations potentially associated with a higher risk of developing complex ventricular arrhythmia and sudden cardiac death. KEY POINTS: • Mitral valve prolapse is a common valve disease potentially associated with complex ventricular arrhythmia and sudden cardiac death. • The mechanism of arrhythmogenesis in mitral valve prolapse is complex and multifactorial, due to the interplay among multiple conditions including valve morphological alteration, mechanical stretch, myocardial structure remodeling with fibrosis, and inflammation. • Cardiac imaging, especially echocardiography and cardiac magnetic resonance, is crucial in the identification of several features associated with the potential risk of serious cardiac events. In particular, cardiac magnetic resonance has the advantage of being able to detect myocardial fibrosis which is currently the strongest prognosticator.
Keywords: Arrhythmogenic mitral valve prolapse; Cardiac imaging technique; Computed tomography; Magnetic resonance; Mitral valve prolapse.
© 2023. The Author(s), under exclusive licence to European Society of Radiology.
Conflict of interest statement
Conflict of interest
Marco Francone is
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. Anna Palmisano is a member of the European Radiology Experimental scientific editorial board.
Figures
References
-
- Sabbag A, Essayagh B, Barrera JDR et al. (2022) EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed cby the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society. EP Europace. 10.1093/europace/euac125 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
