

"De novo replication repair deficient glioblastoma, IDH-wildtype" is a distinct glioblastoma subtype in adults that may benefit from immune checkpoint blockade
- PMID: 38079020
- PMCID: PMC10713691
- DOI: 10.1007/s00401-023-02654-1
"De novo replication repair deficient glioblastoma, IDH-wildtype" is a distinct glioblastoma subtype in adults that may benefit from immune checkpoint blockade
Abstract
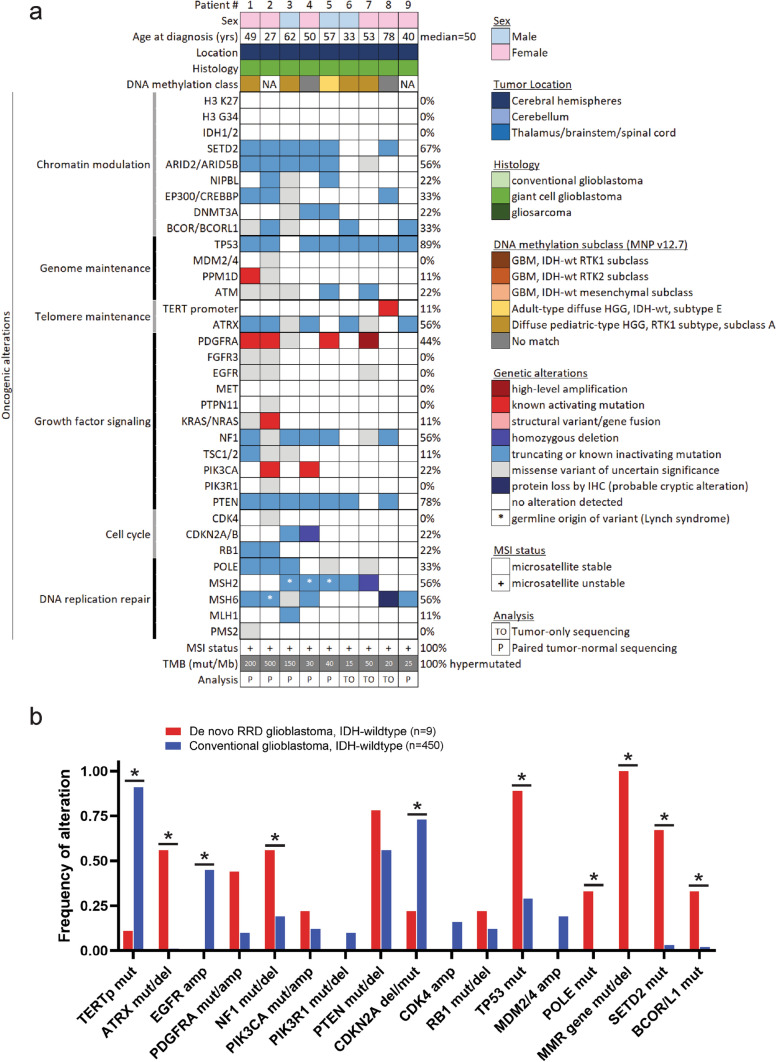
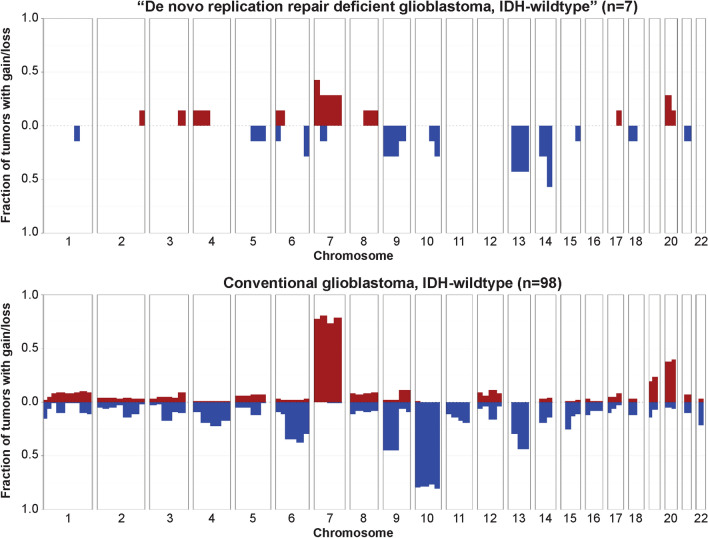
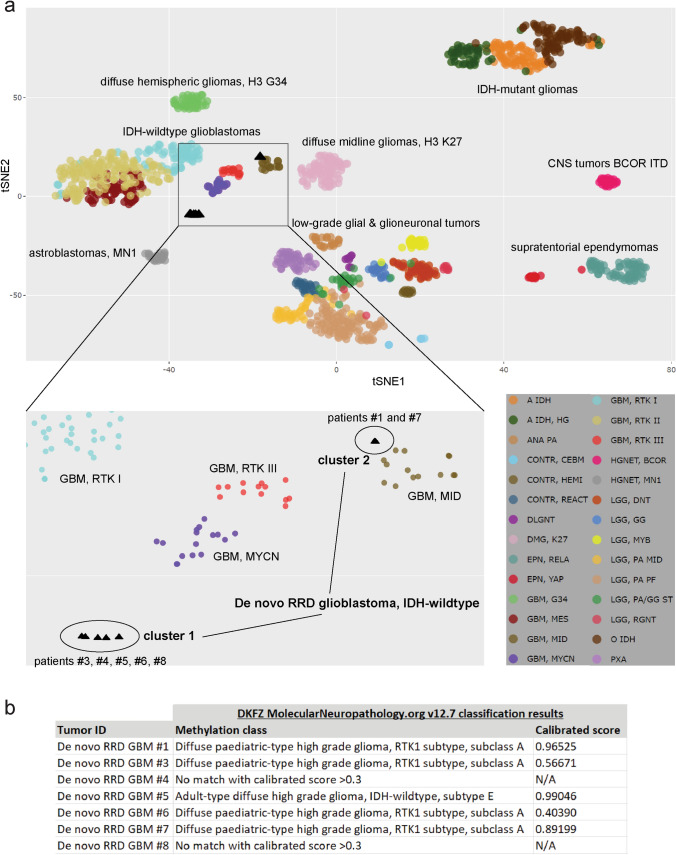
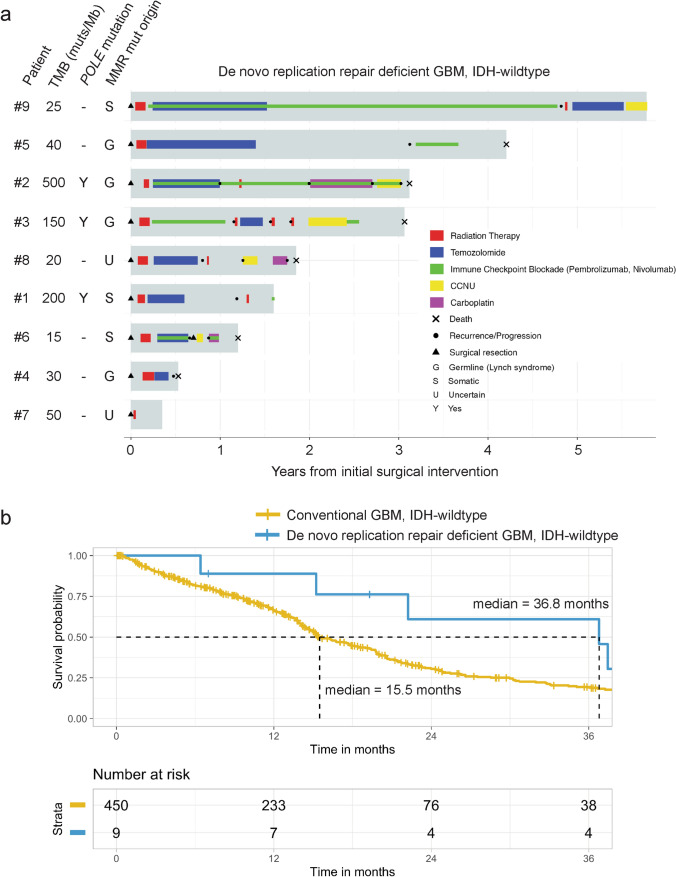
Glioblastoma is a clinically and molecularly heterogeneous disease, and new predictive biomarkers are needed to identify those patients most likely to respond to specific treatments. Through prospective genomic profiling of 459 consecutive primary treatment-naïve IDH-wildtype glioblastomas in adults, we identified a unique subgroup (2%, 9/459) defined by somatic hypermutation and DNA replication repair deficiency due to biallelic inactivation of a canonical mismatch repair gene. The deleterious mutations in mismatch repair genes were often present in the germline in the heterozygous state with somatic inactivation of the remaining allele, consistent with glioblastomas arising due to underlying Lynch syndrome. A subset of tumors had accompanying proofreading domain mutations in the DNA polymerase POLE and resultant "ultrahypermutation". The median age at diagnosis was 50 years (range 27-78), compared with 63 years for the other 450 patients with conventional glioblastoma (p < 0.01). All tumors had histologic features of the giant cell variant of glioblastoma. They lacked EGFR amplification, lacked combined trisomy of chromosome 7 plus monosomy of chromosome 10, and only rarely had TERT promoter mutation or CDKN2A homozygous deletion, which are hallmarks of conventional IDH-wildtype glioblastoma. Instead, they harbored frequent inactivating mutations in TP53, NF1, PTEN, ATRX, and SETD2 and recurrent activating mutations in PDGFRA. DNA methylation profiling revealed they did not align with known reference adult glioblastoma methylation classes, but instead had unique globally hypomethylated epigenomes and mostly classified as "Diffuse pediatric-type high grade glioma, RTK1 subtype, subclass A". Five patients were treated with immune checkpoint blockade, four of whom survived greater than 3 years. The median overall survival was 36.8 months, compared to 15.5 months for the other 450 patients (p < 0.001). We conclude that "De novo replication repair deficient glioblastoma, IDH-wildtype" represents a biologically distinct subtype in the adult population that may benefit from prospective identification and treatment with immune checkpoint blockade.
Keywords: Giant cell glioblastoma; Hypermutation; Immune checkpoint blockade; Immunotherapy; Lynch syndrome; Mismatch repair deficiency; Molecular neuro-oncology; Molecular neuropathology; POLE; Ultrahypermutation.
© 2023. The Author(s).
Conflict of interest statement
D.A.S. and A.P. are members of the editorial board of
Figures



References
-
- Bakry D, Aronson M, Durno C, Rimawi H, Farah R, Alharbi QK, et al. Genetic and clinical determinants of constitutional mismatch repair deficiency syndrome: report from the constitutional mismatch repair deficiency consortium. Eur J Cancer. 2014;50:987–996. doi: 10.1016/j.ejca.2013.12.005. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
