

A non-socially-sensitive predictive model of prostate cancer for Asian males with benign prostatic hyperplasia: A multi-site cross-sectional case-control study
- PMID: 38079423
- PMCID: PMC10712871
- DOI: 10.1371/journal.pone.0295608
A non-socially-sensitive predictive model of prostate cancer for Asian males with benign prostatic hyperplasia: A multi-site cross-sectional case-control study
Abstract
Background: Benign prostatic hyperplasia (BPH) is common in aging Asian males and is associated with an excess risk of developing prostate cancer (PCa). However, discussions about socially-sensitive experiences such as sexual activity, which can significantly predict PCa risk, may be considered stigmatized in Asian culture. This study aimed to develop a predictive model for PCa risk in Asian males with BPH using non-socially-sensitive information.
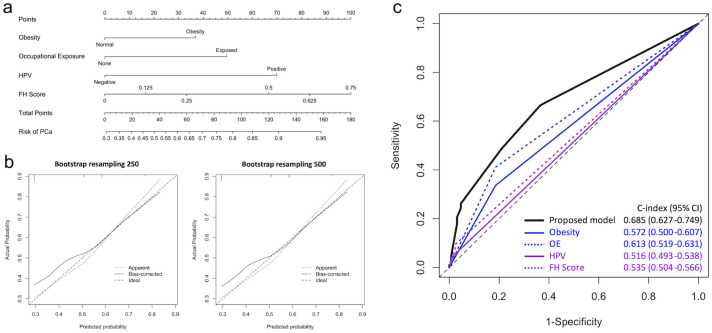
Methods: A cross-sectional case-control study, with PCa patients as the cases and remaining as the controls, was conducted on a cohort of Taiwanese males with BPH from four medical institutions. Patients who met the inclusion criteria were enrolled, excluding those aged over 86 years or who had received human papillomavirus (HPV) vaccination. Non-socially-sensitive variables such as obesity, occupational exposure, HPV infection, and PCa family history score (FH score) were included in a fully adjusted logistic regression model, and depicted using a nomogram.
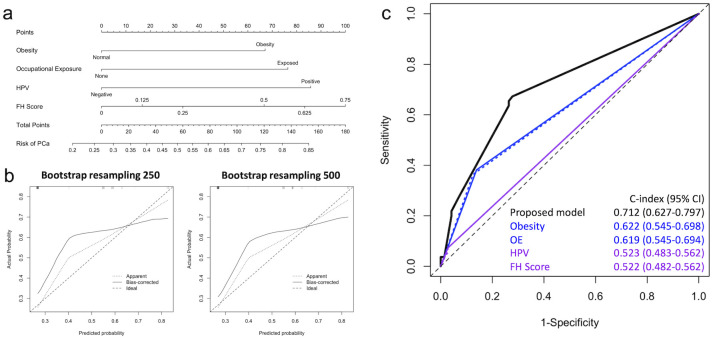
Results: Among 236 BPH patients, 45.3% had PCa. Obesity, occupational exposure, HPV infection, and family history of PCa were significantly associated with PCa risk. The FH score (OR = 1.89, 95% CI = 1.03-3.47, P = 0.041) had the highest impact, followed by HPV infection (OR = 1.47, 95% CI = 1.03-2.11, P = 0.034), occupational exposure (OR = 1.32, 95% CI = 1.15-1.51, P <0.001), and obesity (OR = 1.22, 95% CI = 1.07-1.41, P = 0.005). The nomogram accurately depicted the predictive risk, and the model demonstrated robust performance compared to individual factors. In addition, the subgroup analysis results showed elderly age group could obtain more favorable predictive performance in our proposed model (AUC = 0.712).
Conclusion: This non-socially-sensitive predictive model for PCa risk in Taiwanese males with BPH integrates multiple factors that could provide acceptable PCa risk-predictive performance, especially for elderly BPH patients over 70 years, aiding clinical decision-making and early cancer detection.
Copyright: © 2023 Chang et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
BPH: a tell-tale sign of prostate cancer? Results from the Prostate Cancer and Environment Study (PROtEuS).World J Urol. 2015 Dec;33(12):2063-9. doi: 10.1007/s00345-015-1546-z. Epub 2015 Apr 1. World J Urol. 2015. PMID: 25824539
-
Serum antibodies against genitourinary infectious agents in prostate cancer and benign prostate hyperplasia patients: a case-control study.BMC Cancer. 2011 Feb 3;11:53. doi: 10.1186/1471-2407-11-53. BMC Cancer. 2011. PMID: 21291519 Free PMC article.
-
A matched case-control study in Taiwan to evaluate potential risk factors for prostate cancer.Sci Rep. 2023 Mar 16;13(1):4382. doi: 10.1038/s41598-023-31434-w. Sci Rep. 2023. PMID: 36928374 Free PMC article.
-
The controversial relationship between benign prostatic hyperplasia and prostate cancer: the role of inflammation.Eur Urol. 2011 Jul;60(1):106-17. doi: 10.1016/j.eururo.2011.03.055. Epub 2011 Apr 9. Eur Urol. 2011. PMID: 21497433 Review.
-
Review of the role of androgenic hormones in the epidemiology of benign prostatic hyperplasia and prostate cancer.Urology. 1994 Jun;43(6):892-9. doi: 10.1016/0090-4295(94)90163-5. Urology. 1994. PMID: 7515207 Review.
References
-
- Collaborators GBDBPH. The global, regional, and national burden of benign prostatic hyperplasia in 204 countries and territories from 2000 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Healthy Longev. 2022;3(11):e754–e76. doi: 10.1016/S2666-7568(22)00213-6 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
