

Systematic Review and Meta-Analysis of Seasonal Malaria Chemoprevention
- PMID: 38081050
- PMCID: PMC10793029
- DOI: 10.4269/ajtmh.23-0481
Systematic Review and Meta-Analysis of Seasonal Malaria Chemoprevention
Abstract
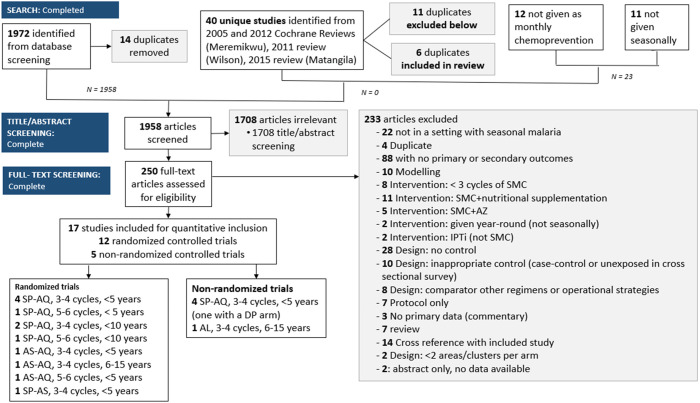
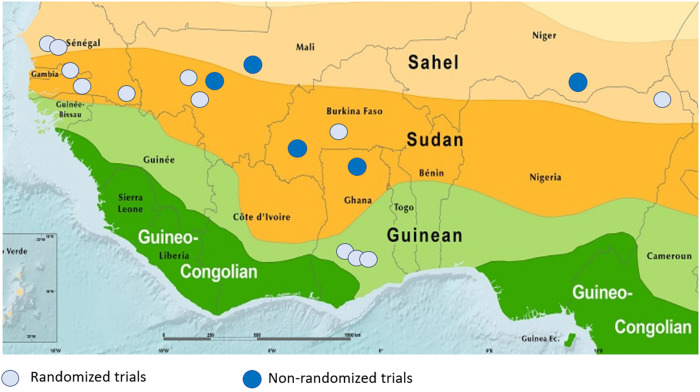
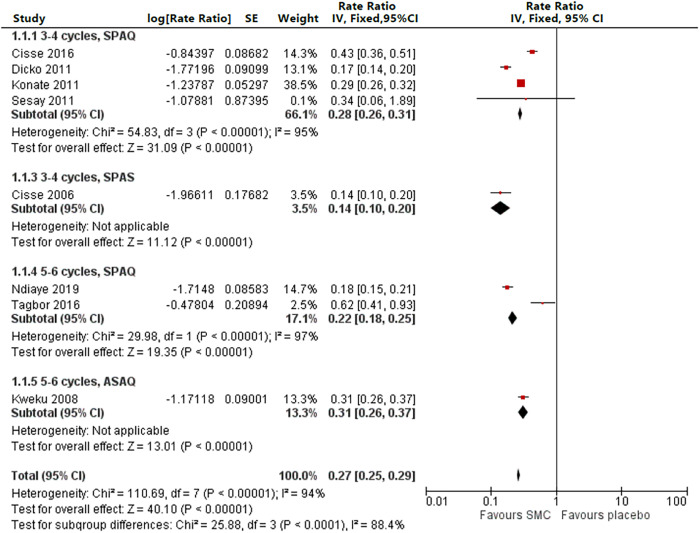
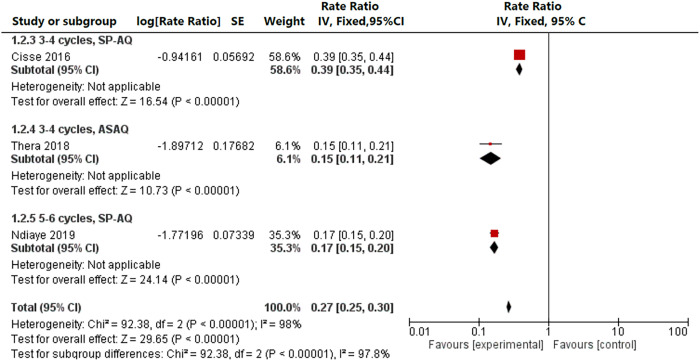
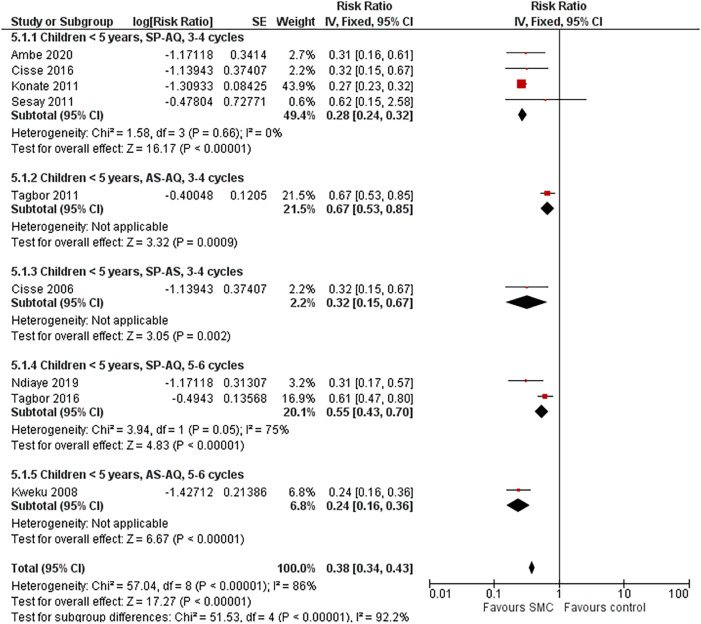
Seasonal malaria chemoprevention (SMC) for children under 5 years of age for up to four monthly cycles during malaria transmission season was recommended by the WHO in 2012 and has been implemented in 13 countries in the Sahel, reaching more than 30 million children annually. Malaria control programs implementing SMC have asked the WHO to consider expanding the age range or number of monthly cycles. We conducted a systematic review and meta-analysis of SMC among children up to 15 years of age and up to six monthly cycles. Twelve randomized studies were included, with outcomes stratified by age (< 5/≥ 5 years), by three or four versus five or six cycles, and by drug where possible. Drug regimens included sulfadoxine-pyrimethamine + amodiaquine, amodiaquine-artesunate, and sulfadoxine-pyrimethamine + artesunate. Included studies were all conducted in Sahelian countries in which high-grade resistance to sulfadoxine-pyrimethamine was rare and in zones with parasite prevalence ranging from 1% to 79%. Seasonal malaria chemoprevention resulted in substantial reductions in uncomplicated malaria incidence measured during that transmission season (rate ratio: 0.27, 95% CI: 0.25-0.29 among children < 5 years; rate ratio: 0.27, 95% CI: 0.25-0.30 among children ≥ 5 years) and in the prevalence of malaria parasitemia measured within 4-6 weeks from the final SMC cycle (risk ratio: 0.38, 95% CI: 0.34-0.43 among children < 5 years; risk ratio: 0.23, 95% CI: 0.11-0.48 among children ≥ 5 years). In high-transmission zones, SMC resulted in a moderately reduced risk of any anemia (risk ratio: 0.77, 95% CI: 0.72-0.83 among children < 5 years; risk ratio: 0.70, 95% CI: 0.52-0.95 among children ≥ 5 years [one study]). Children < 10 years of age had a moderate reduction in severe malaria (risk ratio: 0.53, 95% CI: 0.37-0.76) but no evidence of a mortality reduction. The evidence suggests that in areas in which sulfadoxine-pyrimethamine and amodiaquine remained efficacious, SMC effectively reduced malaria disease burden among children both < 5 and ≥ 5 years old and that the number of cycles should be commensurate with the length of the transmission season, up to six cycles.
Figures
References
-
- World Health Organization , 2019. World Malaria Report 2019. Geneva, Switzerland: WHO.
-
- Etard JF, Le Hesran JY, Diallo A, Diallo JP, Ndiaye JL, Delaunary V, 2004. Childhood mortality and probable causes of death using verbal autopsy in Niakhar, Senegal, 1989–2000. Int J Epidemiol 33: 1286–1292. - PubMed
-
- Jaffar S, Leach A, Greenwood AM, Jepson A, Muller O, Ota MO, Bojang K, Obaro S, Greenwood BM, 1997. Changes in the pattern of infant and childhood mortality in upper river division, the Gambia, from 1989 to 1993. Trop Med Int Health 2: 28–37. - PubMed
-
- World Health Organization , 2012. WHO Policy Recommendation: Seasonal Malaria Chemoprevention (SMC) for Plasmodium falciparum Malaria Control in Highly Seasonal Transmission Areas of the Sahel Sub-Region in Africa. Available at: https://iris.who.int/handle/10665/337978?locale-attribute=en&show=full. Accessed November 13, 2023.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
