

Ankle osteoarthritis: an online survey of current treatment practices of UK-based podiatrists and physiotherapists
- PMID: 38082323
- PMCID: PMC10714609
- DOI: 10.1186/s13047-023-00683-3
Ankle osteoarthritis: an online survey of current treatment practices of UK-based podiatrists and physiotherapists
Abstract
Background: Patients with painful ankle osteoarthritis (OA) have a mixed experience of non-surgical management which they may attribute to a lack of guidance for clinicians on usual care treatment. Therefore, the purpose of this study was to survey the current clinical practices of UK-based physiotherapists and podiatrists for the treatment of painful ankle osteoarthritis (OA).
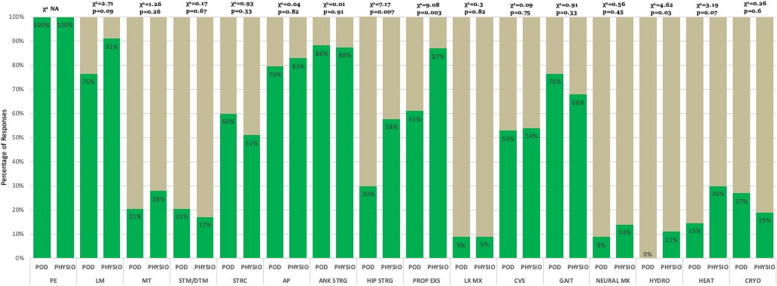
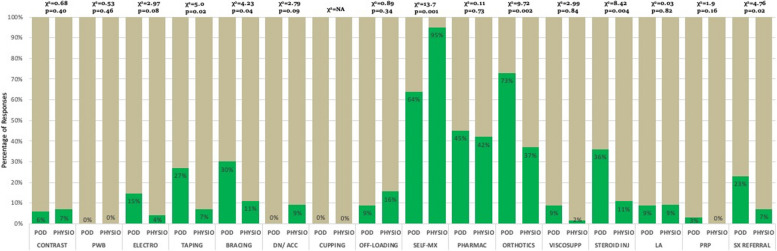
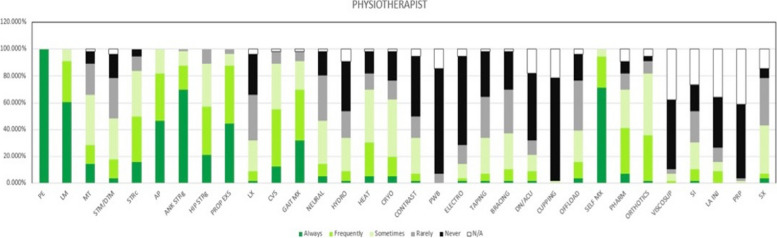
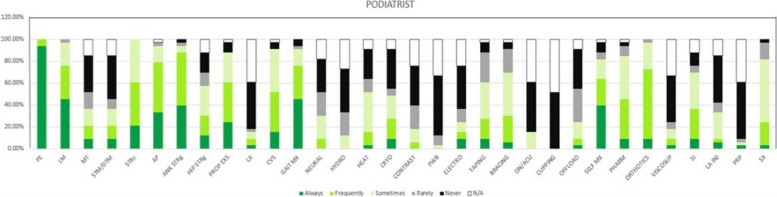
Methods: UK-based physiotherapists and podiatrists who treat patients with ankle OA completed a self-administered online questionnaire about their professional and clinical service characteristics, diagnostic criteria, treatment aims, preferred treatment options, and treatment outcome measures. Data were collected anonymously and stored on JISC online survey. 'Usual care' was defined as a combination of 'Always', and 'Frequently', and 'Not usual care' was defined as 'Sometimes' 'Rarely,' 'Never', and 'not applicable' combined. Statistically significant differences in responses between the physiotherapists and podiatrists were analysed using X2 tests for each treatment modality. Statistical significance was set at p < 0.05.
Results: Between 1st June 2021 and 31st August 2021, 100 responses were received; 2 were invalid. Of the 98 valid responses, 63 were from physiotherapists and 35 from podiatrists. The most common treatment aims in both professions were to reduce pain (n = 87, 89%) and improve quality of life (n = 82, 84%). 50 respondents (51%) offered 3 or 4 treatment sessions and 53 respondents (54%) saw patients for 30-40 min at the first treatment session. The five most common modalities used by physiotherapists were patient education (n = 63, 100%), teaching self-management (n = 58, 92%), lifestyle modification (n = 54, 86%), ankle strengthening (n = 55, 87%), and proprioception exercises (n = 54, 86%). For podiatrists, these were patient education (n = 35, 100%), ankle strengthening (n = 31, 89%), activity pacing (n = 28, 80%), lifestyle modification (n = 27, 77%), and gait training (n = 27, 77%).
Conclusions: This first-ever survey revealed physiotherapists' and podiatrists' current practices to treat painful ankle OA. This study provides a better understanding of how ankle OA is treated in UK current clinical practice and can inform future clinical trials to compare current practice with new treatment modalities.
Keywords: Ankle; Osteoarthritis; Physiotherapy; Podiatry; Survey.
© 2023. The Author(s).
Conflict of interest statement
None of the authors have any competing interests.
Figures
References
-
- Murray C, Marshall M, Rathod T, Bowen CJ, Menz HB, Roddy E. Population prevalence and distribution of ankle pain and symptomatic radiographic ankle osteoarthritis in community dwelling older adults: a systematic review and cross-sectional study. PLoS ONE. 2018;13(4):e0193662. doi: 10.1371/journal.pone.0193662. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
