

Evaluation of the efficacy and safety of amustaline/glutathione pathogen-reduced RBCs in complex cardiac surgery: the Red Cell Pathogen Inactivation (ReCePI) study-protocol for a phase 3, randomized, controlled trial
- PMID: 38082326
- PMCID: PMC10712151
- DOI: 10.1186/s13063-023-07831-x
Evaluation of the efficacy and safety of amustaline/glutathione pathogen-reduced RBCs in complex cardiac surgery: the Red Cell Pathogen Inactivation (ReCePI) study-protocol for a phase 3, randomized, controlled trial
Abstract
Background: Red blood cell (RBC) transfusion is a critical supportive therapy in cardiovascular surgery (CVS). Donor selection and testing have reduced the risk of transfusion-transmitted infections; however, risks remain from bacteria, emerging viruses, pathogens for which testing is not performed and from residual donor leukocytes. Amustaline (S-303)/glutathione (GSH) treatment pathogen reduction technology is designed to inactivate a broad spectrum of infectious agents and leukocytes in RBC concentrates. The ReCePI study is a Phase 3 clinical trial designed to evaluate the efficacy and safety of pathogen-reduced RBCs transfused for acute anemia in CVS compared to conventional RBCs, and to assess the clinical significance of treatment-emergent RBC antibodies.
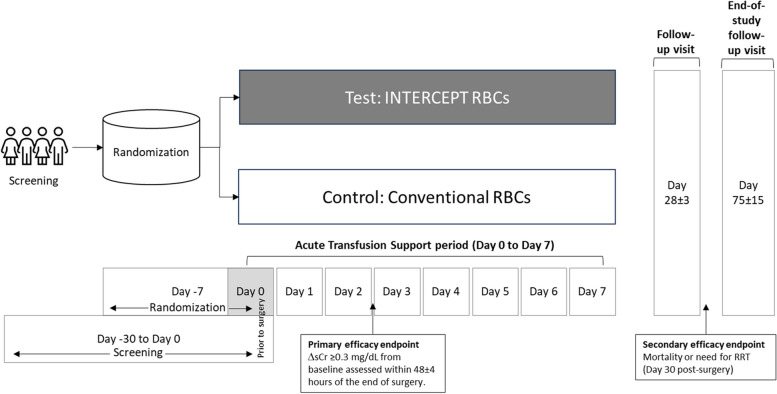
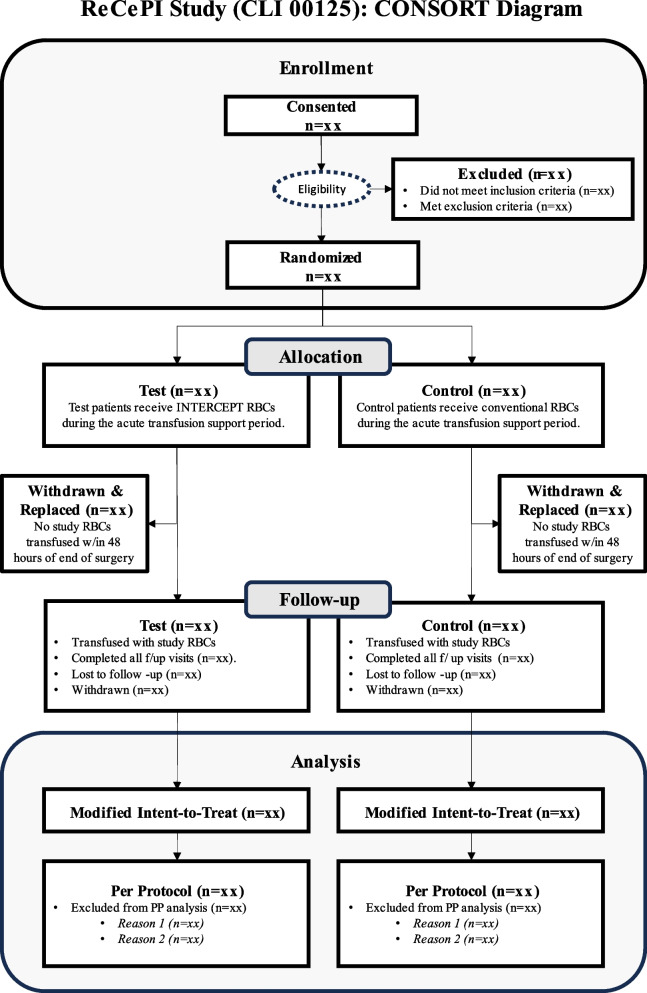
Methods: ReCePI is a prospective, multicenter, randomized, double-blinded, active-controlled, parallel-design, non-inferiority study. Eligible subjects will be randomized up to 7 days before surgery to receive either leukoreduced Test (pathogen reduced) or Control (conventional) RBCs from surgery up to day 7 post-surgery. The primary efficacy endpoint is the proportion of patients transfused with at least one study transfusion with an acute kidney injury (AKI) diagnosis defined as any increased serum creatinine (sCr) level ≥ 0.3 mg/dL (or 26.5 µmol/L) from pre-surgery baseline within 48 ± 4 h of the end of surgery. The primary safety endpoints are the proportion of patients with any treatment-emergent adverse events (TEAEs) related to study RBC transfusion through 28 days, and the proportion of patients with treatment-emergent antibodies with confirmed specificity to pathogen-reduced RBCs through 75 days after the last study transfusion. With ≥ 292 evaluable, transfused patients (> 146 per arm), the study has 80% power to demonstrate non-inferiority, defined as a Test group AKI incidence increase of no more than 50% of the Control group rate, assuming a Control incidence of 30%.
Discussion: RBCs are transfused to prevent tissue hypoxia caused by surgery-induced bleeding and anemia. AKI is a sensitive indicator of renal hypoxia and a novel endpoint for assessing RBC efficacy. The ReCePI study is intended to demonstrate the non-inferiority of pathogen-reduced RBCs to conventional RBCs in the support of renal tissue oxygenation due to acute anemia and to characterize the incidence of treatment-related antibodies to RBCs.
Keywords: Acute kidney injury; Amustaline/GSH; Cardiac surgery; INTERCEPT; Pathogen reduction; Randomized controlled trial; Transfusion-transmitted infections.
© 2023. The Author(s).
Conflict of interest statement
RJB, KL, SB, JPP, NM, LC, and JV are employees and shareholders of Cerus Corporation equity, the Sponsor of the study. The investigators are independent of the Sponsor and declare no relevant conflict of interest. ELS, MES, IJW, YT, NRS, TMB, JPRP, JDG, JSM, RMS, RGP, GAN, RS, TBR, AK, RD, TS, PB, and IL-P are site investigators on the study, receive no compensation from the Sponsor and declare no conflicts relating to the study.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
