

Analysis of risk factors for axial symptoms after posterior cervical open-door laminoplasty
- PMID: 38082364
- PMCID: PMC10714461
- DOI: 10.1186/s13018-023-04426-9
Analysis of risk factors for axial symptoms after posterior cervical open-door laminoplasty
Abstract
Background: Laminoplasty (LP), a procedure commonly used to treat cervical spondylotic myelopathy (CSM), often results in the development of axial symptoms (AS) postoperatively. This study aims to analyze the risk factors associated with the occurrence of AS after LP.
Methods: We collected and evaluated clinical data from 264 patients with CSM who underwent LP treatment at our institution from January 2018 to January 2022 through a single-center retrospective study. Of the patients, 153 were male and 111 were female, with an average age of 58.1 ± 6.7 years. All patients underwent C3-7 posterior laminoplasty. Based on the occurrence of postoperative axial symptoms, the patients were divided into an AS group and a non-AS group. General information, including age, gender, disease duration, Japanese Orthopaedic Association (JOA) score, postoperation early function training, and collar-wearing time, was recorded and compared between the two groups. Surgical-related data, such as operative segments, surgical time, intraoperative blood loss, intraoperative facet joint destruction, and destruction of the C7 spinous process muscle insertion, were also compared. Imaging data, including preoperative cervical curvature, cervical range of motion, preoperative encroachment rate of the anterior spinal canal, and angle of laminar opening, were collected. Univariate and multivariate logistic regression analyses were used to identify risk factors for the development of AS after LP, and receiver operator characteristic (ROC) curves were utilized to explore the optimal preoperative parameters.
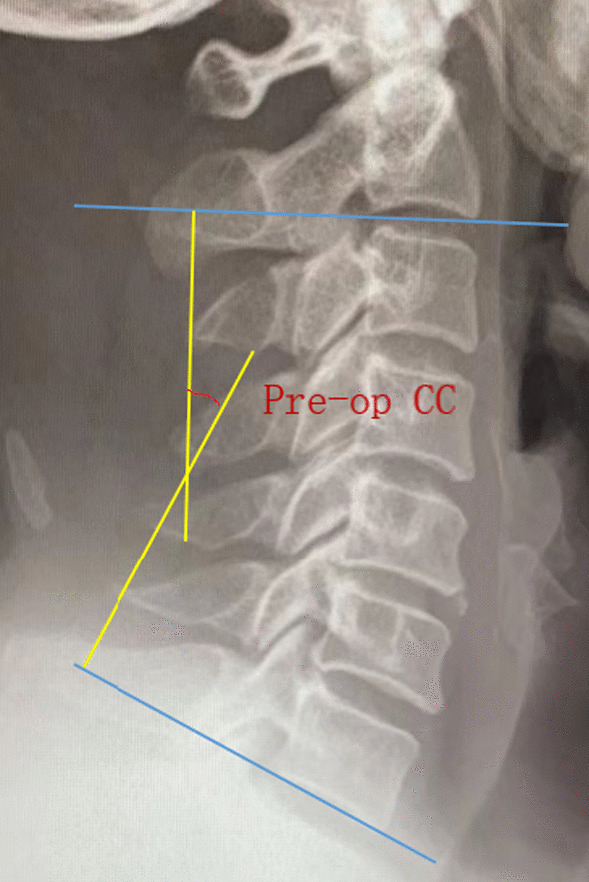
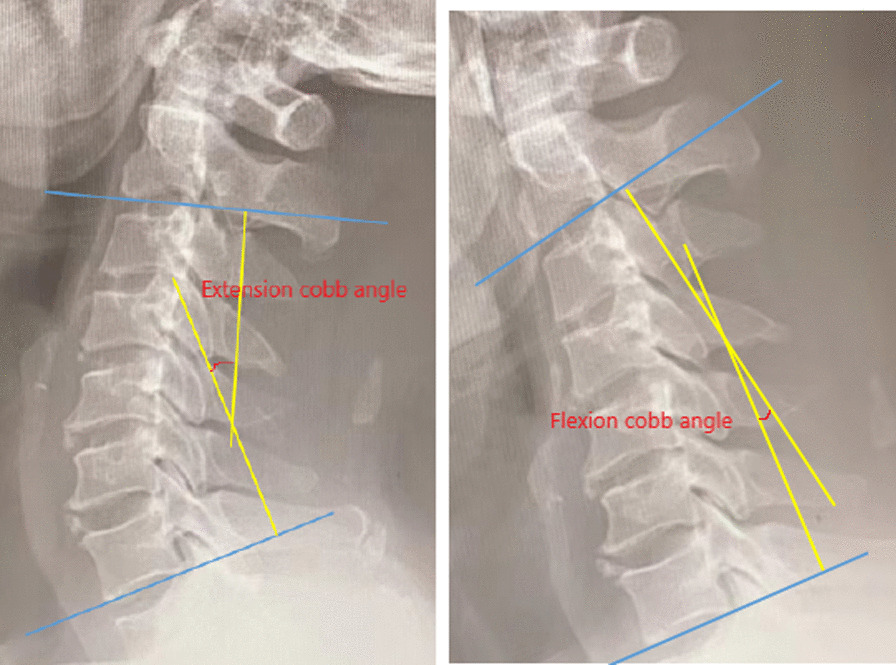
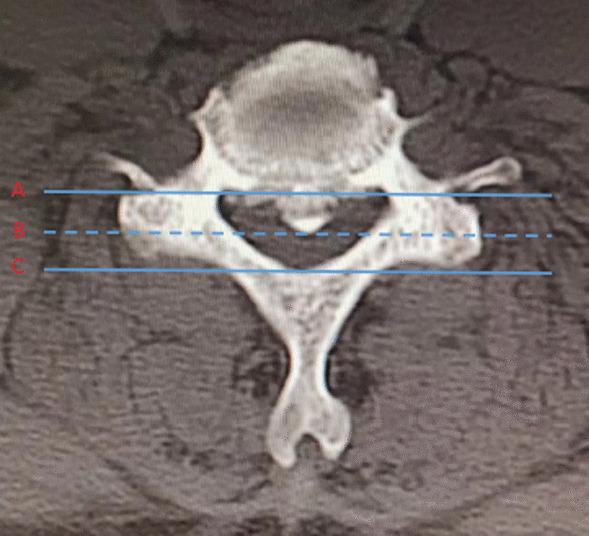
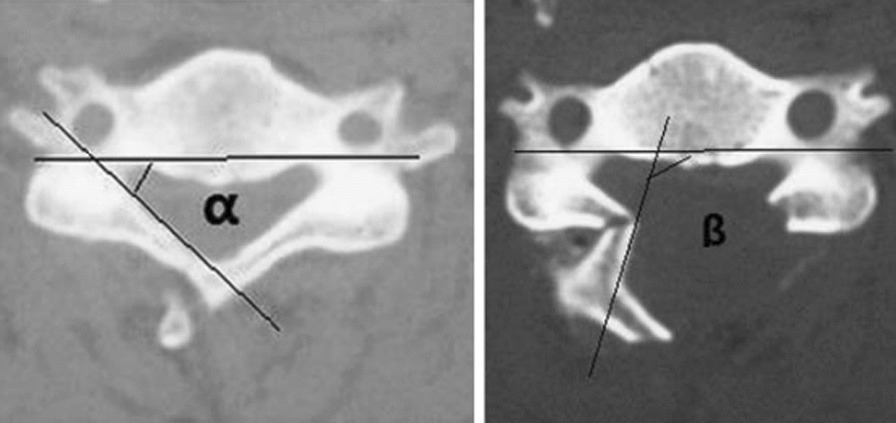
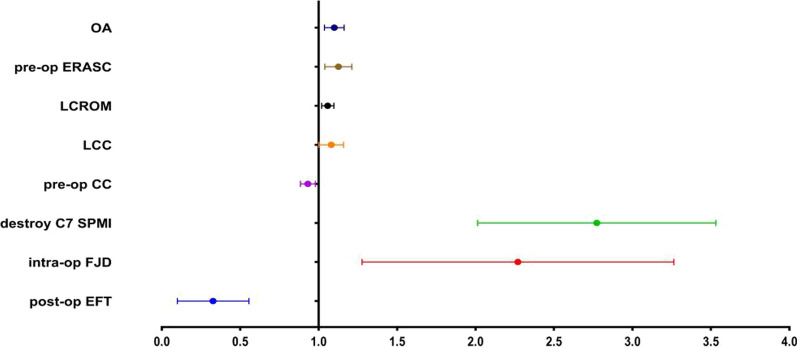
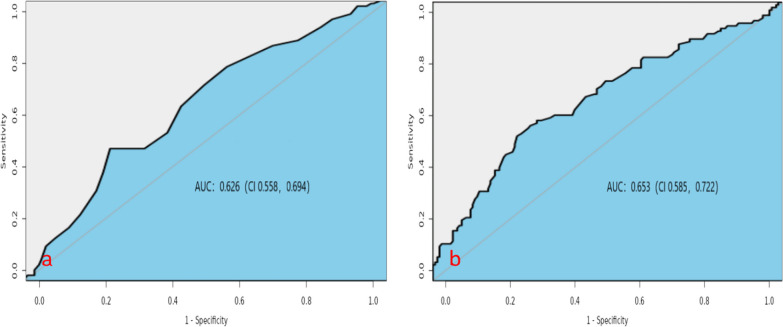
Results: All 264 patients successfully underwent surgery and were followed up for an average of 19.5 ± 6.8 months. At the 6-month follow-up, 117 patients were diagnosed with AS, resulting in an incidence rate of 40.2%. The multivariate logistic regression analysis identified that preoperative encroachment rate of anterior spinal canal (Pre-op ERASC), intraoperative facet joints destruction (Intra-op FJD), intraoperative open-door angle (Intra-op OA), destroy the C7 spinous process muscle insertion (Destroy C7 SPMI), postoperative loss of cervical curvature (Post-op LCC), and postoperative loss of cervical range of motion (Post-op LCROM) were independent risk factors for AS. Conversely, preoperative cervical curvature (Pre-op CC) and postoperation early function training (Post-op EFT) were protective factors against AS. According to the ROC curve, the cutoff values for preoperative anterior spinal canal occupation rate and preoperative cervical curvature were 28.5% and 16.5°, respectively. When the preoperative anterior spinal canal occupation rate was greater than 28.5% or the preoperative cervical curvature was less than 16.5°, AS was more likely to occur after surgery.
Conclusion: High preoperative anterior spinal canal occupation rate, facet joint damage during surgery, C7 spinous process muscle stop point damage, larger angle of laminar opening, and greater postoperative cervical curvature loss and cervical range of motion loss are associated with an increased risk of developing AS after cervical laminoplasty. Conversely, a larger preoperative cervical curvature and early postoperative functional exercises can help reduce the occurrence of AS.
Keywords: Axial symptoms; Cervical spondylotic myelopathy; Cutoff value; Laminoplasty; Risk factors.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Comment in
-
Letter to the editor regarding: risk factors for axial symptoms following laminoplasty for cervical spondylotic myelopathy.J Orthop Surg Res. 2024 Jan 3;19(1):18. doi: 10.1186/s13018-023-04508-8. J Orthop Surg Res. 2024. PMID: 38167447 Free PMC article. No abstract available.
Similar articles
-
Incidence and Risk Factors for the Development of Axial Symptoms Following Posterior Single-Door Laminoplasty: A Retrospective Analysis.World Neurosurg. 2024 Mar;183:e603-e612. doi: 10.1016/j.wneu.2023.12.153. Epub 2024 Jan 5. World Neurosurg. 2024. PMID: 38185458
-
Clinical and Radiographic Outcomes of Modified Unilateral Open-door Laminoplasty with Posterior Muscle-Ligament Complex Preservation for Cervical Spondylotic Myelopathy.Spine (Phila Pa 1976). 2019 Dec 15;44(24):1697-1704. doi: 10.1097/BRS.0000000000003158. Spine (Phila Pa 1976). 2019. PMID: 31794507
-
[Analysis of risk factors of axial symptoms after single door laminoplasty for cervical myelopathy].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2014 May;28(5):620-4. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2014. PMID: 25073285 Chinese.
-
Expansion of Spinal Canal with Lift-Open Laminoplasty: A New Method for Compression Cervical Myelopathy.Orthop Surg. 2021 Jul;13(5):1673-1681. doi: 10.1111/os.13026. Epub 2021 Jun 10. Orthop Surg. 2021. PMID: 34109741 Free PMC article. Review.
-
Is laminoplasty or laminectomy the best strategy for C3 segment in French-door laminoplasty? A systematic review and meta-analysis.J Orthop Surg Res. 2021 Sep 14;16(1):557. doi: 10.1186/s13018-021-02596-y. J Orthop Surg Res. 2021. PMID: 34521434 Free PMC article.
Cited by
-
Efficacy and safety of laminoplasty combined with C3 laminectomy for patients with multilevel degenerative cervical myelopathy: a systematic review and meta-analysis.Eur Spine J. 2024 Oct;33(10):3915-3932. doi: 10.1007/s00586-024-08444-x. Epub 2024 Aug 9. Eur Spine J. 2024. PMID: 39122847
-
A stacking ensemble machine learning model for predicting postoperative axial pain intensity in patients with degenerative cervical myelopathy.Sci Rep. 2025 Mar 22;15(1):9954. doi: 10.1038/s41598-025-94755-y. Sci Rep. 2025. PMID: 40121328 Free PMC article.
-
Pre- and Intraoperative Factors Associated With Improvement of Neck Pain After Laminoplasty for the Treatment of Cervical Myelopathy.Global Spine J. 2025 Jan 15;15(6):21925682251314490. doi: 10.1177/21925682251314490. Online ahead of print. Global Spine J. 2025. PMID: 39812366 Free PMC article.
-
Traditional Chinese Medicine treatment for postoperative axial symptoms of cervical spondylotic myelopathy: a systematic review.BMJ Open. 2024 Oct 23;14(10):e085050. doi: 10.1136/bmjopen-2024-085050. BMJ Open. 2024. PMID: 39448215 Free PMC article.
-
Letter to the editor regarding: risk factors for axial symptoms following laminoplasty for cervical spondylotic myelopathy.J Orthop Surg Res. 2024 Jan 3;19(1):18. doi: 10.1186/s13018-023-04508-8. J Orthop Surg Res. 2024. PMID: 38167447 Free PMC article. No abstract available.
References
-
- Montano N, Ricciardi L, Olivi A. Comparison of anterior cervical decompression and fusion versus laminoplasty in the treatment of multilevel cervical spondylotic myelopathy: a meta-analysis of clinical and radiological outcomes. World Neurosurg. 2019;130:530–536.e2. doi: 10.1016/j.wneu.2019.06.144. - DOI - PubMed
-
- Yoshii T, Sakai K, Hirai T, et al. Anterior decompression with fusion versus posterior decompression with fusion for massive cervical ossification of the posterior longitudinal ligament with a ≥50% canal occupying ratio: a multicenter retrospective study. Spine J. 2016;16(11):1351–1357. doi: 10.1016/j.spinee.2016.07.532. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
