

Machine learning for the prediction of sepsis-related death: a systematic review and meta-analysis
- PMID: 38082381
- PMCID: PMC10712076
- DOI: 10.1186/s12911-023-02383-1
Machine learning for the prediction of sepsis-related death: a systematic review and meta-analysis
Abstract
Background and objectives: Sepsis is accompanied by a considerably high risk of mortality in the short term, despite the availability of recommended mortality risk assessment tools. However, these risk assessment tools seem to have limited predictive value. With the gradual integration of machine learning into clinical practice, some researchers have attempted to employ machine learning for early mortality risk prediction in sepsis patients. Nevertheless, there is a lack of comprehensive understanding regarding the construction of predictive variables using machine learning and the value of various machine learning methods. Thus, we carried out this systematic review and meta-analysis to explore the predictive value of machine learning for sepsis-related death at different time points.
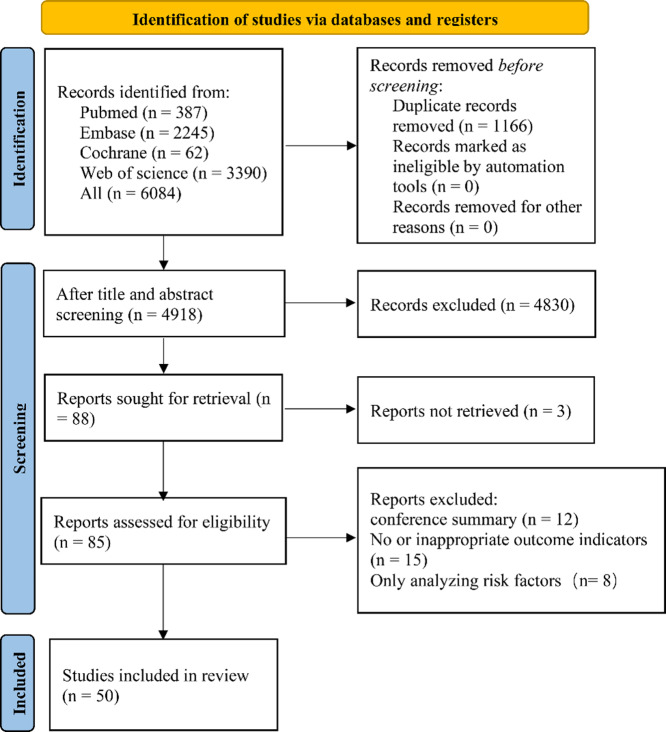
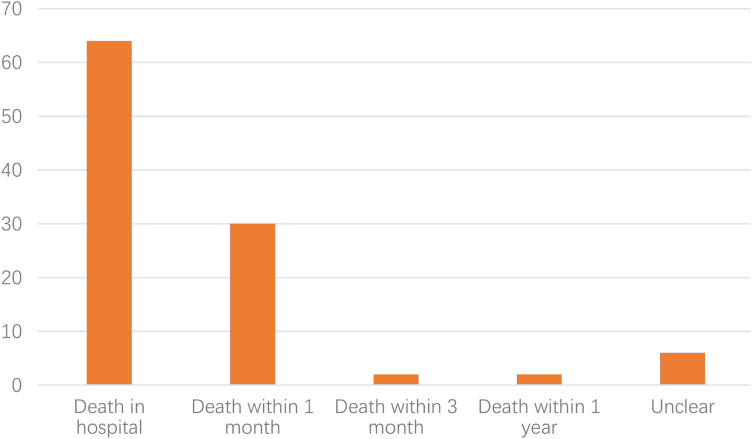
Methods: PubMed, Embase, Cochrane, and Web of Science databases were searched until August 9th, 2022. The risk of bias in predictive models was assessed using the Prediction model Risk of Bias Assessment Tool (PROBAST). We also performed subgroup analysis according to time of death and type of model and summarized current predictive variables used to construct models for sepsis death prediction.
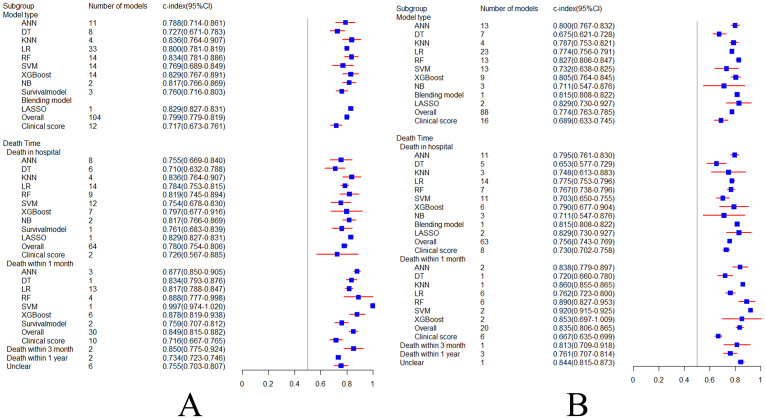
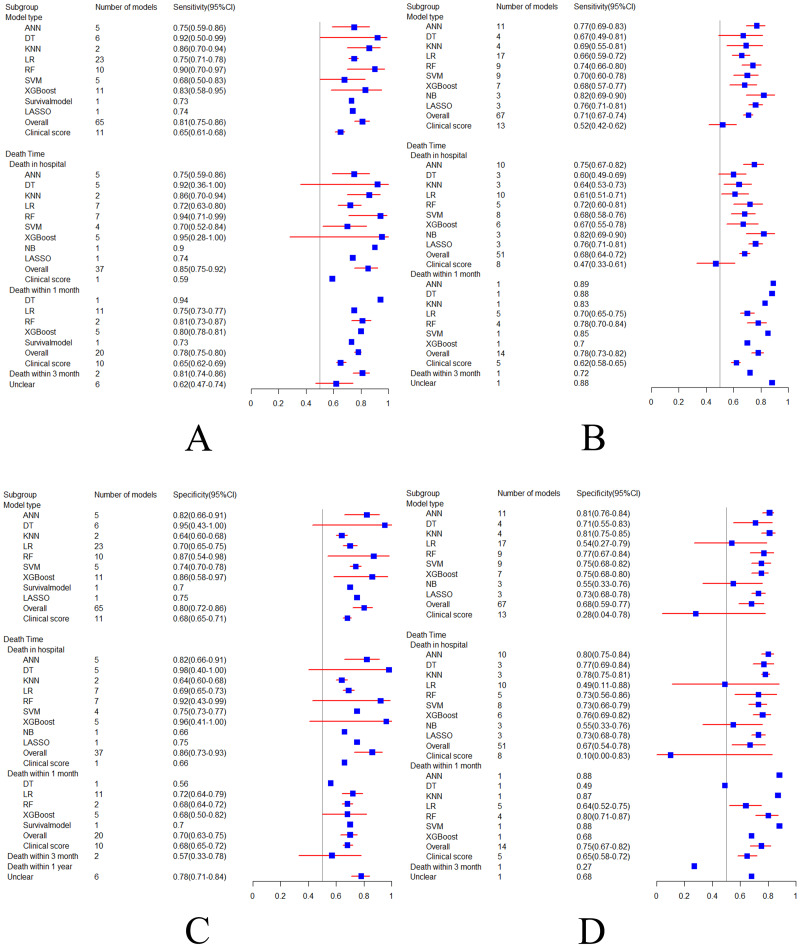
Results: Fifty original studies were included, covering 104 models. The combined Concordance index (C-index), sensitivity, and specificity of machine learning models were 0.799, 0.81, and 0.80 in the training set, and 0.774, 0.71, and 0.68 in the validation set, respectively. Machine learning outperformed conventional clinical scoring tools and showed excellent C-index, sensitivity, and specificity in different subgroups. Random Forest (RF) and eXtreme Gradient Boosting (XGBoost) are the preferred machine learning models because they showed more favorable accuracy with similar modeling variables. This study found that lactate was the most frequent predictor but was seriously ignored by current clinical scoring tools.
Conclusion: Machine learning methods demonstrate relatively favorable accuracy in predicting the mortality risk in sepsis patients. Given the limitations in accuracy and applicability of existing prediction scoring systems, there is an opportunity to explore updates based on existing machine learning approaches. Specifically, it is essential to develop or update more suitable mortality risk assessment tools based on the specific contexts of use, such as emergency departments, general wards, and intensive care units.
Keywords: Machine learning; Meta-analysis; Mortality; Sepsis; Systematic review.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, Angus DC, Reinhart K. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259–72. doi: 10.1164/rccm.201504-0781OC. - DOI - PubMed
-
- Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, Colombara DV, Ikuta KS, Kissoon N, Finfer S, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of Disease Study. Lancet (London England) 2020;395(10219):200–11. doi: 10.1016/S0140-6736(19)32989-7. - DOI - PMC - PubMed
-
- Vincent JL, Marshall JC, Namendys-Silva SA, François B, Martin-Loeches I, Lipman J, Reinhart K, Antonelli M, Pickkers P, Njimi H, et al. Assessment of the worldwide burden of critical Illness: the intensive care over nations (ICON) audit. The Lancet Respiratory Medicine. 2014;2(5):380–6. doi: 10.1016/S2213-2600(14)70061-X. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
