

Implementation strategies for hospital-based probiotic administration in a stepped-wedge cluster randomized trial design for preventing hospital-acquired Clostridioides difficile infection
- PMID: 38082421
- PMCID: PMC10714625
- DOI: 10.1186/s12913-023-10350-9
Implementation strategies for hospital-based probiotic administration in a stepped-wedge cluster randomized trial design for preventing hospital-acquired Clostridioides difficile infection
Abstract
Background: Clostridioides difficile infection (CDI) is associated with considerable morbidity and mortality in hospitalized patients, especially among older adults. Probiotics have been evaluated to prevent hospital-acquired (HA) CDI in patients who are receiving systemic antibiotics, but the implementation of timely probiotic administration remains a challenge. We evaluated methods for effective probiotic implementation across a large health region as part of a study to assess the real-world effectiveness of a probiotic to prevent HA-CDI (Prevent CDI-55 +).
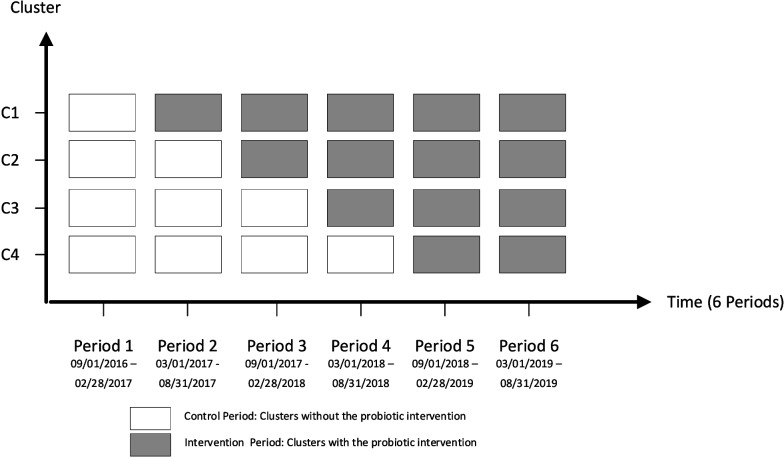
Methods: We used a stepped-wedge cluster-randomized controlled trial across four acute-care adult hospitals (n = 2,490 beds) to implement the use of the probiotic Bio-K + ® (Lactobacillus acidophilus CL1285®, L. casei LBC80R® and L. rhamnosus CLR2®; Laval, Quebec, Canada) in patients 55 years and older receiving systemic antimicrobials. The multifaceted probiotic implementation strategy included electronic clinical decision support, local site champions, and both health care provider and patient educational interventions. Focus groups were conducted during study implementation to identify ongoing barriers and facilitators to probiotic implementation, guiding needed adaptations of the implementation strategy. Focus groups were thematically analyzed using the Theoretical Domains Framework and the Consolidated Framework of Implementation Research.
Results: A total of 340 education sessions with over 1,800 key partners and participants occurred before and during implementation in each of the four hospitals. Site champions were identified for each included hospital, and both electronic clinical decision support and printed educational resources were available to health care providers and patients. A total of 15 individuals participated in 2 focus group and 7 interviews. Key barriers identified from the focus groups resulted in adaptation of the electronic clinical decision support and the addition of nursing education related to probiotic administration. As a result of modifying implementation strategies for identified behaviour change barriers, probiotic adherence rates were from 66.7 to 75.8% at 72 h of starting antibiotic therapy across the four participating acute care hospitals.
Conclusions: Use of a barrier-targeted multifaceted approach, including electronic clinical decision support, education, focus groups to guide the adaptation of the implementation plan, and local site champions, resulted in a high probiotic adherence rate in the Prevent CDI-55 + study.
Keywords: Focus group; Hospital-acquired Clostridioides difficile Infection; Order entry; Probiotics; Protocol implementation.
© 2023. The Author(s).
Conflict of interest statement
TL and OEL receive industry research funding from Finch Therapeutics, Rebiotix Inc, Crestone Inc, Artugen Therapeutics, Seres Therapeutics, ImmuniMed Inc, MGB Biopharma, Summit Therapeutics and Vedanta Biosciences for clinical trials of C.
Figures
References
-
- Leal JR, Conly J, Weaver R, Wick J, Henderson EA, Manns B, et al. Attributable costs and length of stay of hospital-acquired Clostridioides difficile: a population-based matched cohort study in Alberta, Canada. Infect Control Hosp Epidemiol. 2019;40(10):1135–1143. doi: 10.1017/ice.2019.178. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
