

Single-cell profiling reveals preferential reduction of memory B cell subsets in cladribine patients that correlates with treatment response
- PMID: 38084102
- PMCID: PMC10710756
- DOI: 10.1177/17562864231211077
Single-cell profiling reveals preferential reduction of memory B cell subsets in cladribine patients that correlates with treatment response
Abstract
Background: Cladribine is a highly effective immunotherapy that is applied in two short-term courses over 2 years and reduces relapse rate and disease progression in patients with relapsing multiple sclerosis (MS). Despite the short treatment period, cladribine has a long-lasting effect on disease activity even after recovery of lymphocyte counts, suggesting a yet undefined long-term immune modulating effect.
Objectives: Our aim was to provide a more profound understanding of the detailed effects of cladribine, also with regard to the patients' therapy response.
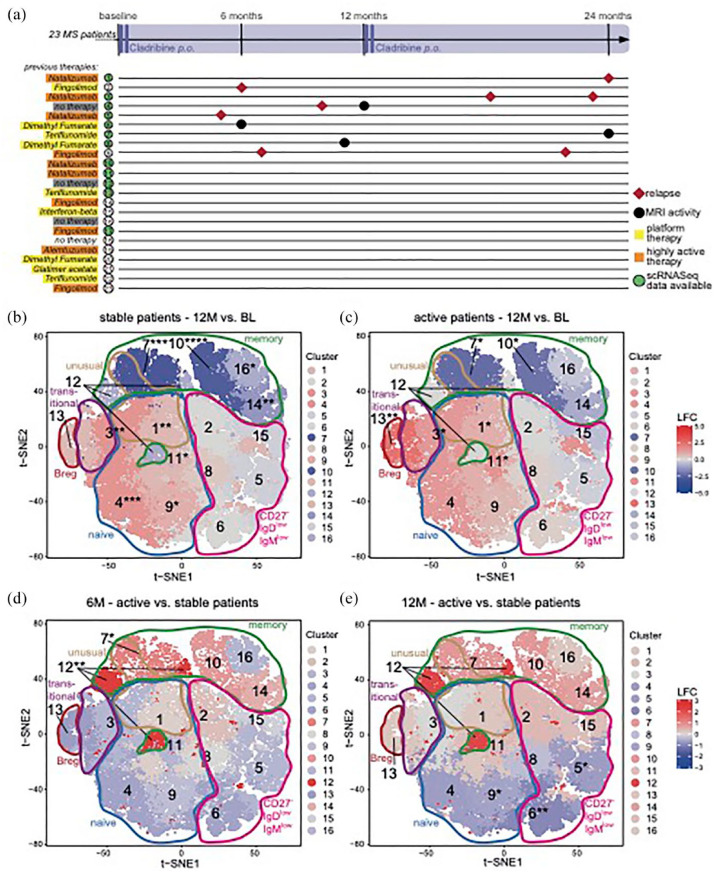
Design: We performed an open-labeled, explorative, prospective, single-arm study, in which we examined the detailed lymphocyte subset development of MS patients who received cladribine treatment over 2 years.
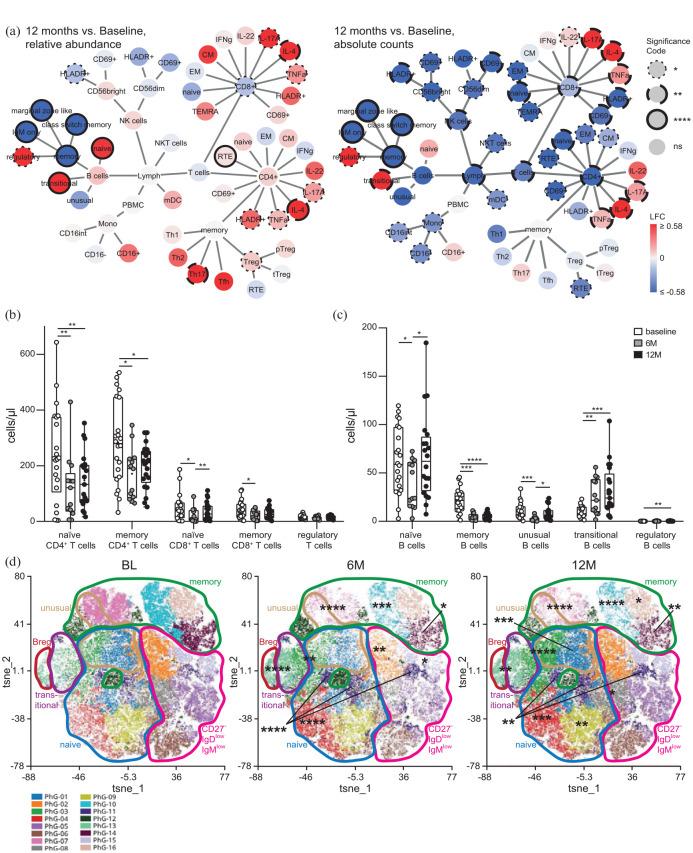
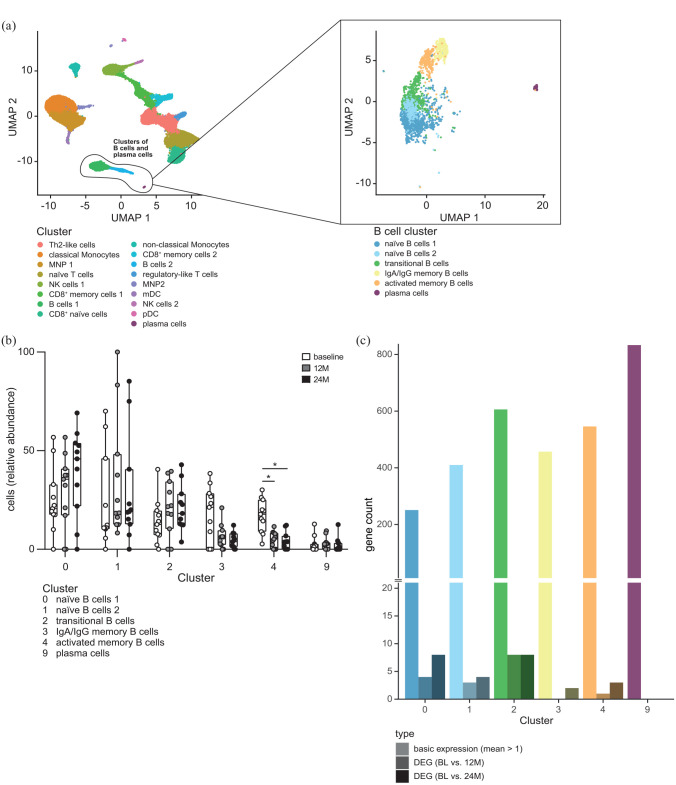
Methods: We performed in-depth profiling of the effects of cladribine on peripheral blood lymphocytes by flow cytometry, bulk RNA sequencing of sorted CD4+ T cells, CD8+ T cells, and CD19+ B cells as well as single-cell RNA sequencing of peripheral blood mononuclear cells in a total of 23 MS patients before and at different time points up to 24 months after cladribine treatment. Data were correlated with clinical and cranial magnetic resonance imaging (MRI) disease activity.
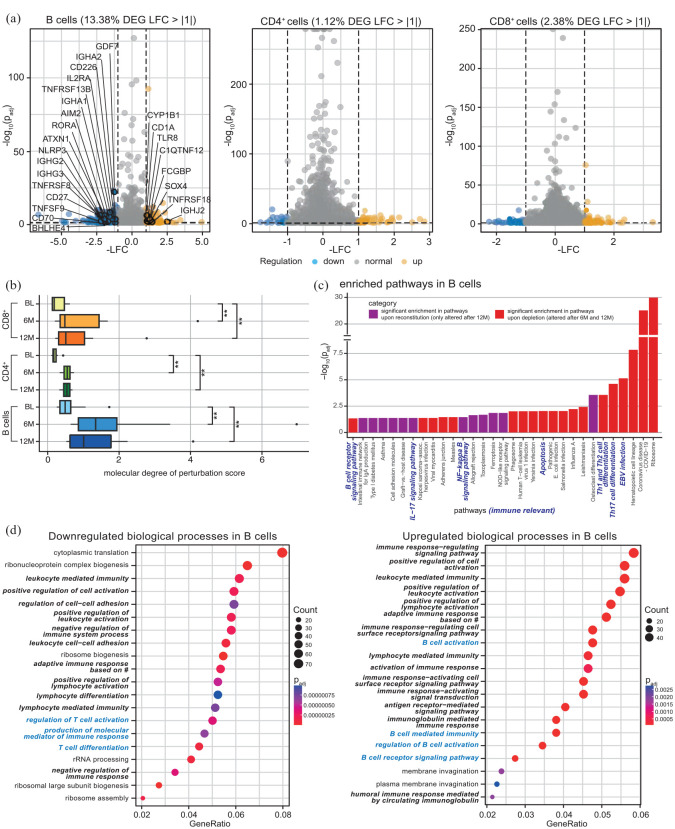
Results: Flow cytometry revealed a predominant and sustained reduction of memory B cells compared to other B cell subsets after cladribine treatment, whereas T cell subsets were slightly reduced in a more uniform pattern. The overall transcriptional profile of total blood B cells exhibited reduced expression of proinflammatory and T cell activating genes, while single-cell transcriptomics revealed that gene expression within each B cell cluster did not change over time. Stable patients displayed stronger reductions of selected memory B cell clusters as compared to patients with clinical or cerebral MRI disease activity.
Conclusion: We describe a pronounced and sustained effect of cladribine on the memory B cell compartment, and the resulting change in B cell subset composition causes a significant alteration of B cell transcriptional profiles resulting in reduced proinflammatory and T cell activating capacities. The extent of reduction in selected memory B cell clusters by cladribine may predict treatment response.
Keywords: cladribine; memory B cells; multiple sclerosis.
© The Author(s), 2023.
Figures
References
-
- Dendrou C, Fugger L, Friese M. Immunopathology of multiple sclerosis. Nat Rev Immunol 2015; 15: 545–558. - PubMed
-
- Hohlfeld R, Dornmair K, Meinl E, et al.. The search for the target antigens of multiple sclerosis, part 1: autoreactive CD4+ T lymphocytes as pathogenic effectors and therapeutic targets. Lancet Neurol 2016; 15: 198–209. - PubMed
-
- Leist T, Weissert R. Cladribine: mode of action and implications for treatment of multiple sclerosis. Clin Neuropharmacol 2011; 34: 28–35. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
