

Early identification of delayed wound healing in complex diabetic foot ulcers treated with a dermal regeneration template: a novel clinical target and its risk factors
- PMID: 38085826
- PMCID: PMC10871583
- DOI: 10.1097/JS9.0000000000000898
Early identification of delayed wound healing in complex diabetic foot ulcers treated with a dermal regeneration template: a novel clinical target and its risk factors
Abstract
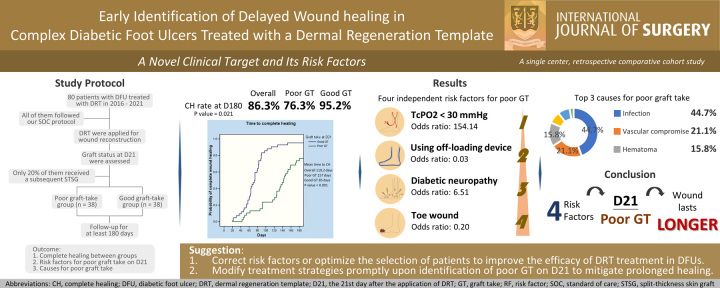
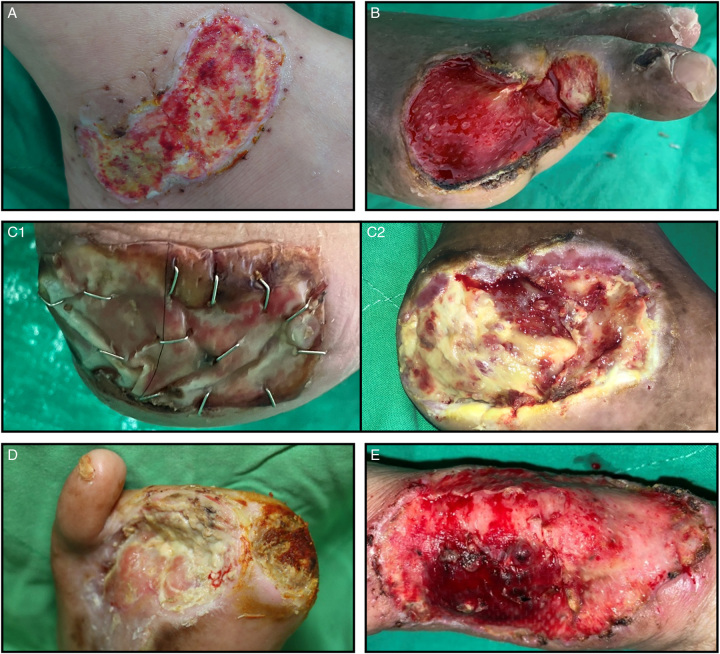
Background: The dermal regeneration template (DRT), a tissue-engineered skin substitute composing a permanent dermal matrix and an upper temporary silicone layer that serves as the epidermis, has demonstrated efficacy in treating uncomplicated diabetic foot ulcers (DFUs). Our institution has obtained good outcomes with DRT in patients with more complicated DFUs. Because of its chronicity, the authors are working to identify a clinical target that anticipates delayed healing early in the treatment in addition to determining the risk factors linked to this endpoint to increase prevention.
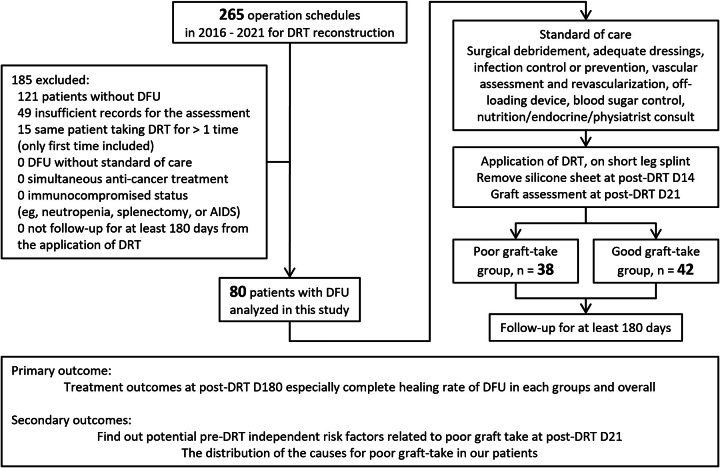
Materials and methods: This retrospective single-center study analyzed patients with DFUs who underwent wound reconstruction using DRT between 2016 and 2021. The patients were categorized into poor or good graft-take groups based on their DRT status on the 21st day after the application. Their relationship with complete healing (CH) rate at day 180 was analyzed. Variables were collected for risk factors for poor graft take at day 21. Independent risk factors were identified after multivariable analysis. The causes of poor graft take were also reported.
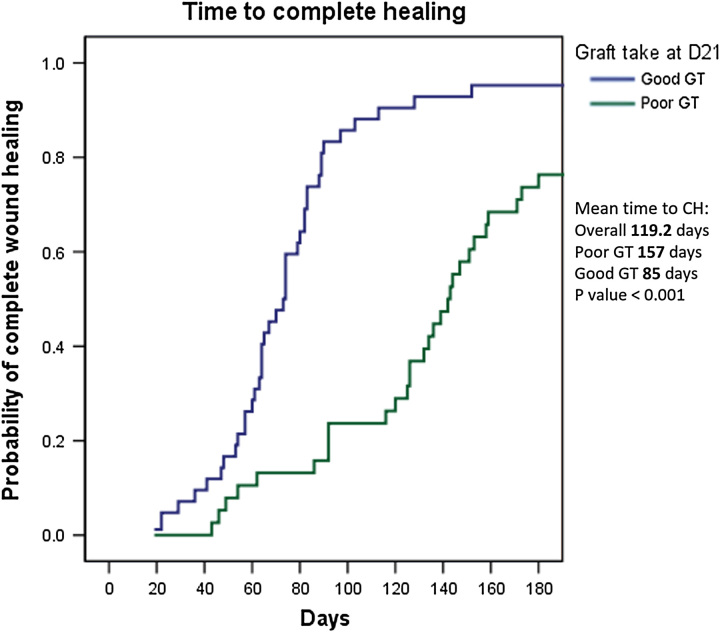
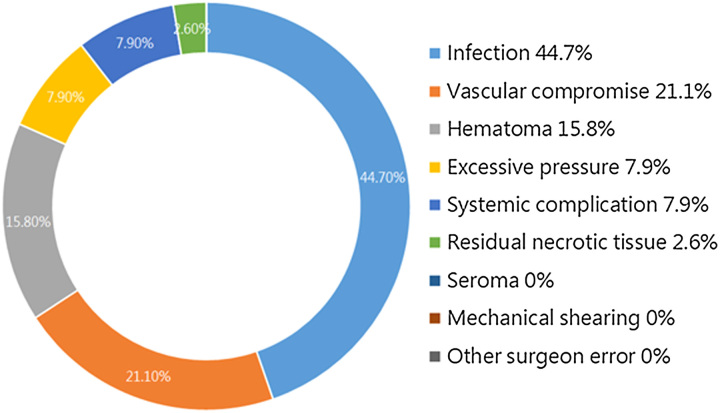
Results: This study examined 80 patients (38 and 42 patients in the poor and good graft-take groups, respectively). On day 180, the CH rate was 86.3% overall, but the poor graft-take group had a significantly lower CH rate (76.3 vs. 95.2%, P =0.021) than the good graft-take group. Our analysis identified four independent risk factors: transcutaneous oxygen pressure less than 30 mmHg (odds ratio, 154.14), off-loading device usage (0.03), diabetic neuropathy (6.51), and toe wound (0.20). The most frequent cause of poor graft take was infection (44.7%), followed by vascular compromise (21.1%) and hematoma (15.8%).
Conclusion: Our study introduces the novel concept of poor graft take at day 21 associated with delayed wound healing. Four independent risk factors were identified, which allows physicians to arrange interventions to mitigate their effects or select patients more precisely. DRT represents a viable alternative to address DFUs, even in complicated wounds. A subsequent split-thickness skin graft is not always necessary to achieve CH.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
All authors in this research have no financial or personal relationships with other people or Organizations that could inappropriately influence our work.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures

References
-
- Zhang P, Lu J, Jing Y, et al. . Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis. Ann Med 2017;49:106–116. - PubMed
-
- Uccioli L, Izzo V, Meloni M, et al. . Non-healing foot ulcers in diabetic patients: general and local interfering conditions and management options with advanced wound dressings. J Wound Care 2015;24(suppl 4):35–42. - PubMed
-
- Moxey PW, Gogalniceanu P, Hinchliffe RJ, et al. . Lower extremity amputations — a review of global variability in incidence. Diabet Med 2011;28:1144–1153. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
