

Tailoring and Evaluating Treatment with the Patient-Specific Needs Evaluation: A Patient-Centered Approach
- PMID: 38085953
- PMCID: PMC11412570
- DOI: 10.1097/PRS.0000000000011199
Tailoring and Evaluating Treatment with the Patient-Specific Needs Evaluation: A Patient-Centered Approach
Abstract
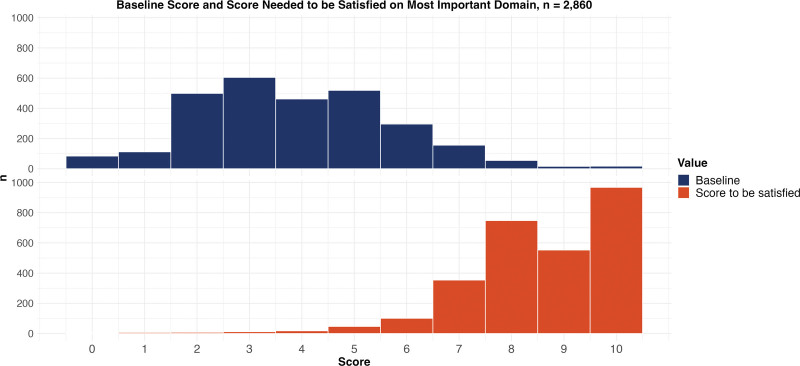
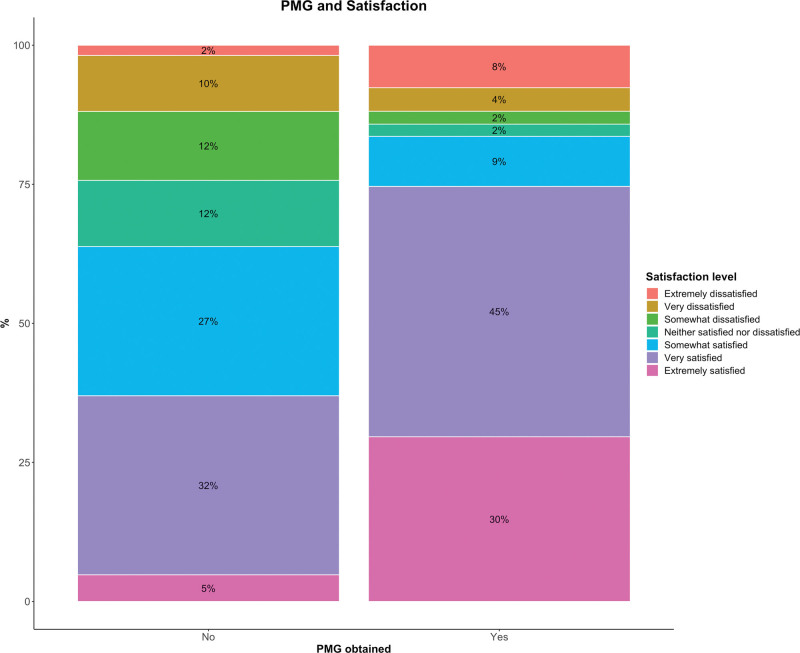
Background: No patient-reported instrument assesses patient-specific information needs, treatment goals, and personal meaningful gain (PMG), a novel construct evaluating individualized, clinically relevant improvement. This study reports the development of the Patient-Specific Needs Evaluation (PSN) and examines its discriminative validity (ie, its ability to distinguish satisfied from dissatisfied patients) and test-retest reliability in patients with hand or wrist conditions.
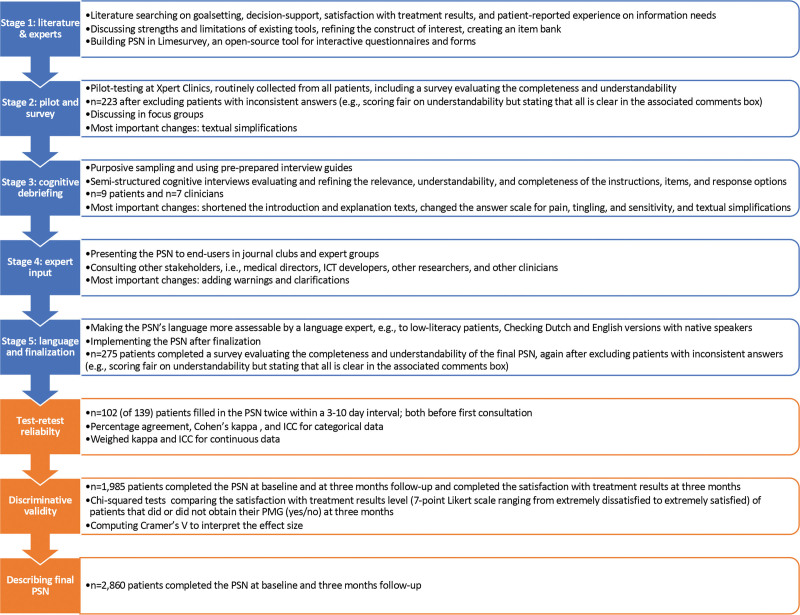
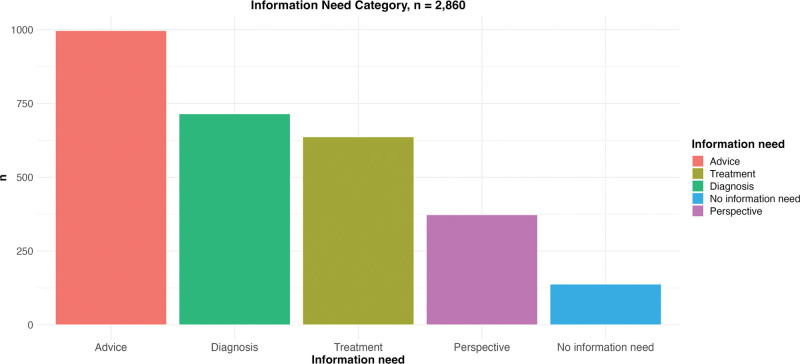
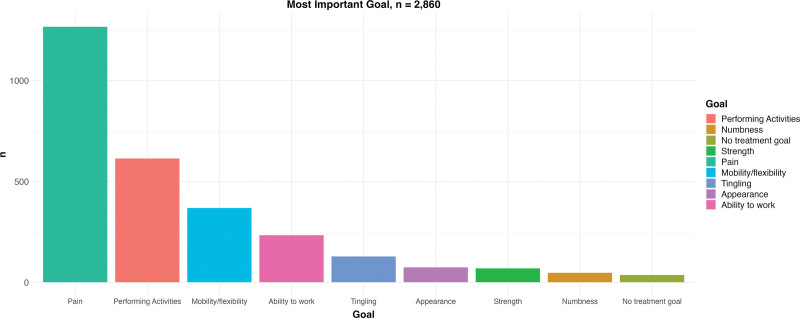
Methods: A mixed-methods approach was used to develop and validate the PSN, following Consensus-Based Standards for the Selection of Health Measurement Instruments guidelines, including pilot testing, a survey (pilot, n = 223; final PSN, n = 275), cognitive debriefing ( n = 16), expert input, and validation. Discriminative validity was assessed by comparing the satisfaction level of patients who did and did not achieve their PMG ( n = 1985) and test-retest reliability using absolute agreement, the Cohen kappa, and intraclass correlation coefficients ( n = 102). The authors used a sample of 2860 patients to describe responses to the final PSN.
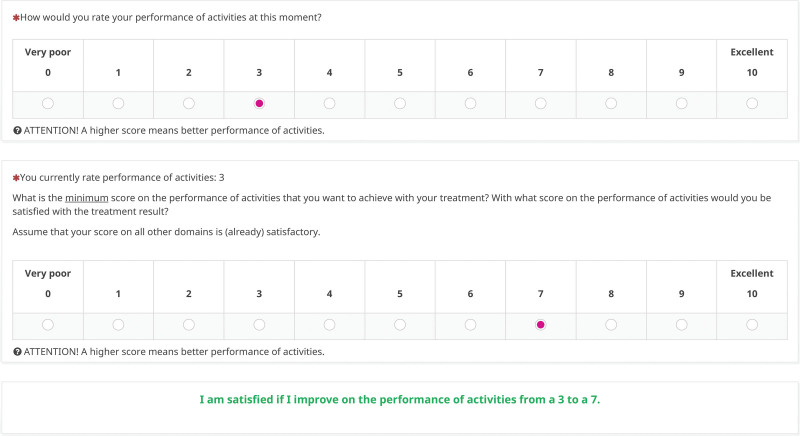
Results: The PSN has only 5 questions (completion time, ±3 minutes) and is freely accessible online. The items and response options were considered understandable by 90% to 92% of the end-users and complete by 84% to 89%. The PSN had excellent discriminative validity (Cramer V, 0.48; P < 0.001) and moderate to high test-retest reliability (kappa, 0.46 to 0.68; intraclass correlation coefficients, 0.53 to 0.73).
Conclusions: The PSN is a freely available, patient-centered decision support tool that helps clinicians tailor their consultations to patients' individual needs and goals. It contains the PMG, a novel construct evaluating individualized, clinically relevant treatment outcomes. The PSN may function as a conversation starter, facilitate expectation management, and aid shared decision-making. The PSN is implementation-ready and can be readily adapted to other patient populations.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the American Society of Plastic Surgeons.
Conflict of interest statement
Dr. Wouters received funding from ZonMw to support this research. The remaining authors have no conflicting interests in relation to the work presented in this article.
Figures
References
-
- Porter ME. What is value in health care? N Engl J Med. 2010;363:2477–2481. - PubMed
-
- Barry MJ, Edgman-Levitan S. Shared decision making: the pinnacle of patient-centered care. N Engl J Med. 2012;366:780–781. - PubMed
-
- Basch E. Patient-reported outcomes: harnessing patients’ voices to improve clinical care. N Engl J Med. 2017;376:105–108. - PubMed
-
- Bernstein DN, Calfee RP, Hammert WC, Rozental TD, Witkowski ML, Porter ME. Value-based health care in hand surgery: where are we & where do we go from here? J Hand Surg. 2022;47:999–1004. - PubMed
-
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press; 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
