

Trigeminal nerve stimulation: a current state-of-the-art review
- PMID: 38087375
- PMCID: PMC10717521
- DOI: 10.1186/s42234-023-00128-z
Trigeminal nerve stimulation: a current state-of-the-art review
Abstract
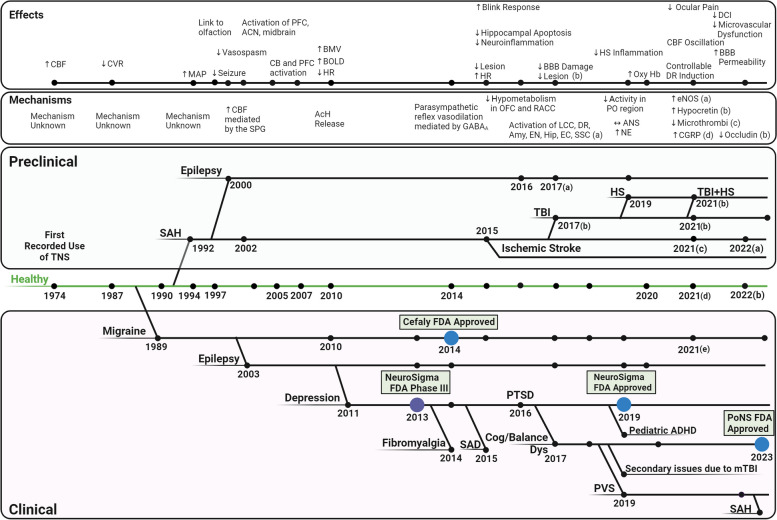
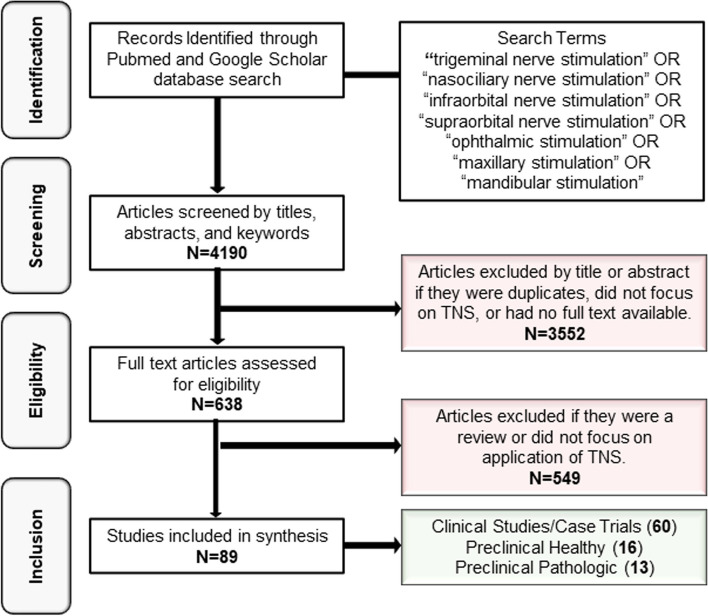
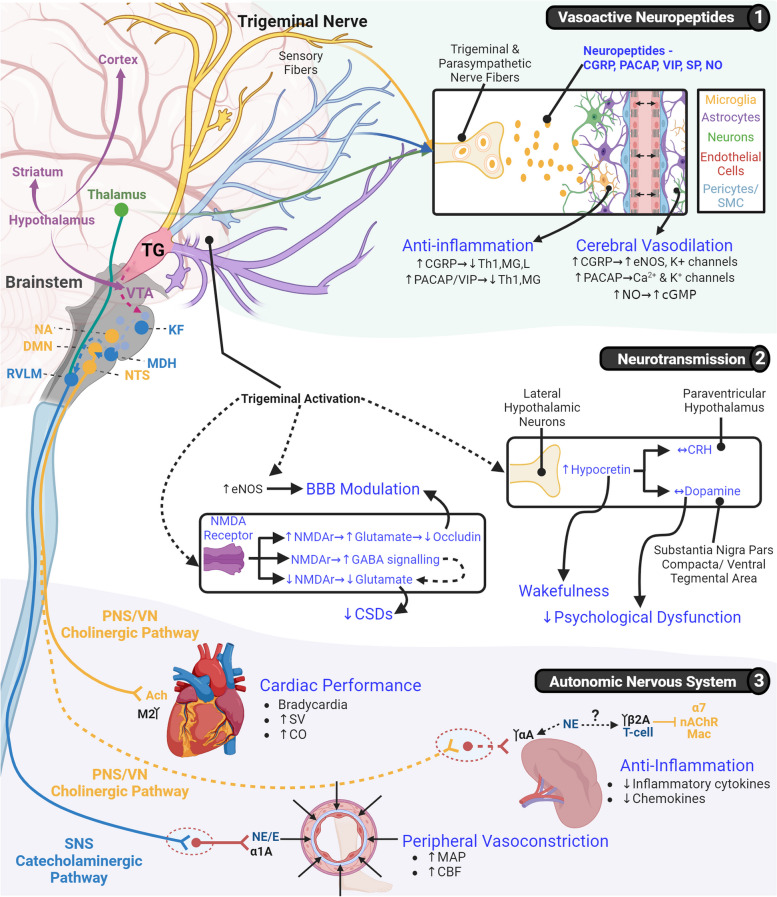
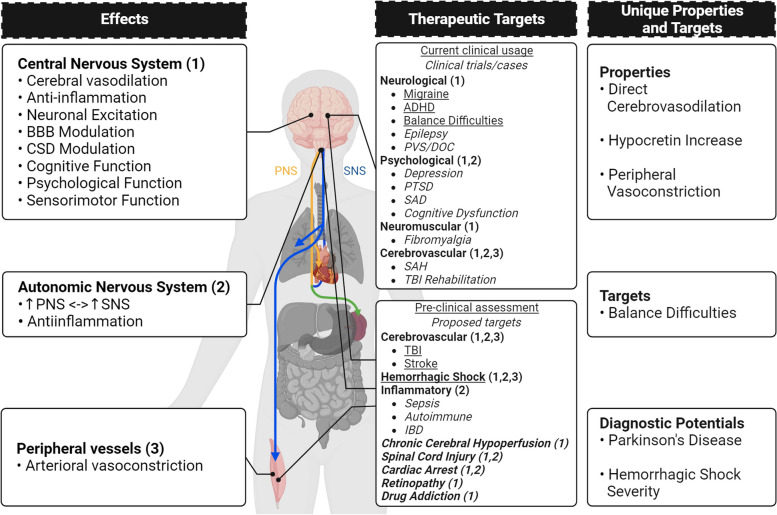
Nearly 5 decades ago, the effect of trigeminal nerve stimulation (TNS) on cerebral blood flow was observed for the first time. This implication directly led to further investigations and TNS' success as a therapeutic intervention. Possessing unique connections with key brain and brainstem regions, TNS has been observed to modulate cerebral vasodilation, brain metabolism, cerebral autoregulation, cerebral and systemic inflammation, and the autonomic nervous system. The unique range of effects make it a prime therapeutic modality and have led to its clinical usage in chronic conditions such as migraine, prolonged disorders of consciousness, and depression. This review aims to present a comprehensive overview of TNS research and its broader therapeutic potentialities. For the purpose of this review, PubMed and Google Scholar were searched from inception to August 28, 2023 to identify a total of 89 relevant studies, both clinical and pre-clinical. TNS harnesses the release of vasoactive neuropeptides, modulation of neurotransmission, and direct action upon the autonomic nervous system to generate a suite of powerful multitarget therapeutic effects. While TNS has been applied clinically to chronic pathological conditions, these powerful effects have recently shown great potential in a number of acute/traumatic pathologies. However, there are still key mechanistic and methodologic knowledge gaps to be solved to make TNS a viable therapeutic option in wider clinical settings. These include bimodal or paradoxical effects and mechanisms, questions regarding its safety in acute/traumatic conditions, the development of more selective stimulation methods to avoid potential maladaptive effects, and its connection to the diving reflex, a trigeminally-mediated protective endogenous reflex. The address of these questions could overcome the current limitations and allow TNS to be applied therapeutically to an innumerable number of pathologies, such that it now stands at the precipice of becoming a ground-breaking therapeutic modality.
Keywords: Autonomic nervous system; Bioelectronic medicine; Cerebral blood flow; Cerebral vasodilation; Diving reflex; Neuromodulation; Neurotransmission; Trigeminal nerve; Trigeminal nerve stimulation; Vasoactive neuropeptide.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Arias DE, Buneo CA. Effects of kilohertz electrical stimulation of the trigeminal nerve on motor learning. Annu Int Conf IEEE Eng Med Biol Soc. 2022;2022:5103–5106. - PubMed
-
- Atalay B, Bolay H, Dalkara T, Soylemezoglu F, Oge K, Ozcan OE. Transcorneal stimulation of trigeminal nerve afferents to increase cerebral blood flow in rats with cerebral vasospasm: a noninvasive method to activate the trigeminovascular reflex. J Neurosurg. 2002;97(5):1179–1183. doi: 10.3171/jns.2002.97.5.1179. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources