

Systematic Evaluation of Clinical, Nutritional, and Fecal Microbial Factors for Their Association With Colorectal Polyps
- PMID: 38088370
- PMCID: PMC10887443
- DOI: 10.14309/ctg.0000000000000660
Systematic Evaluation of Clinical, Nutritional, and Fecal Microbial Factors for Their Association With Colorectal Polyps
Abstract
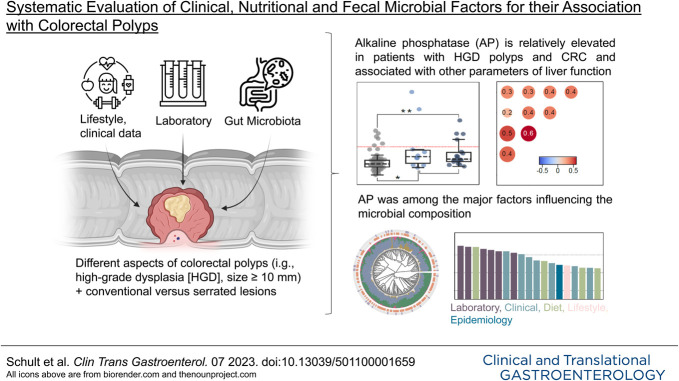
Introduction: The identification of risk factors for precursor lesions of colorectal cancer (CRC) holds great promise in the context of prevention. With this study, we aimed to identify patient characteristics associated with colorectal polyps (CPs) and polyp features of potential malignant progression. Furthermore, a potential association with gut microbiota in this context was investigated.
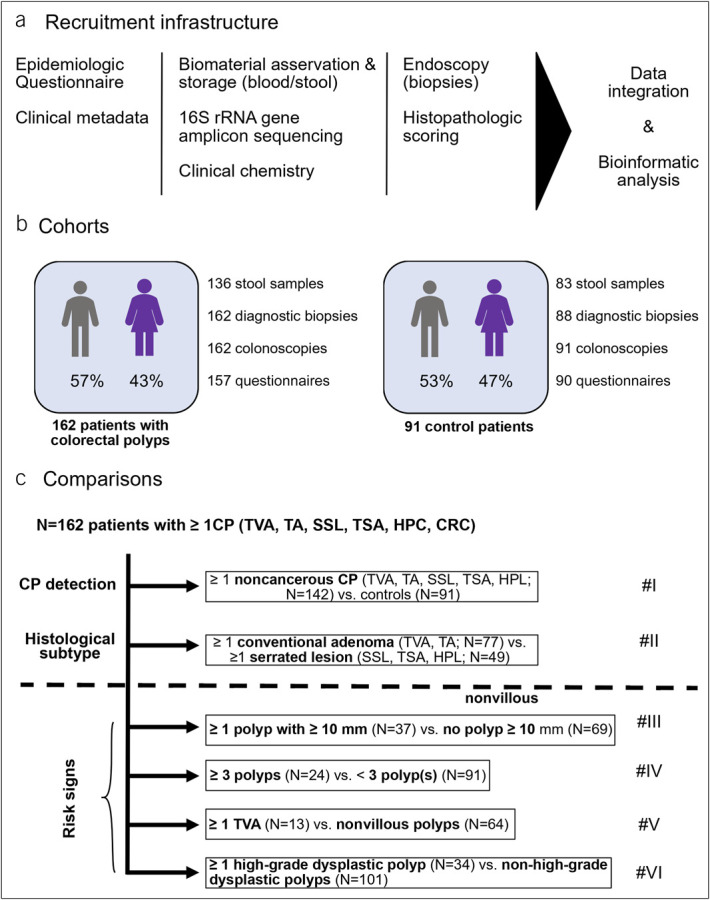
Methods: In this single-center study, a total of 162 patients with CPs and 91 control patients were included. Multiple variables including information on lifestyle, diet, serum parameters, and gut microbiota, analyzed by 16S-rRNA gene amplicon sequencing and functional imputations (Picrust2), were related to different aspects of CPs.
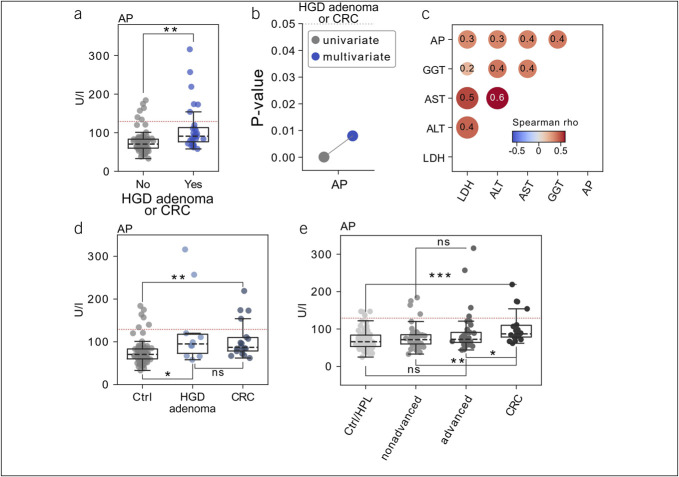
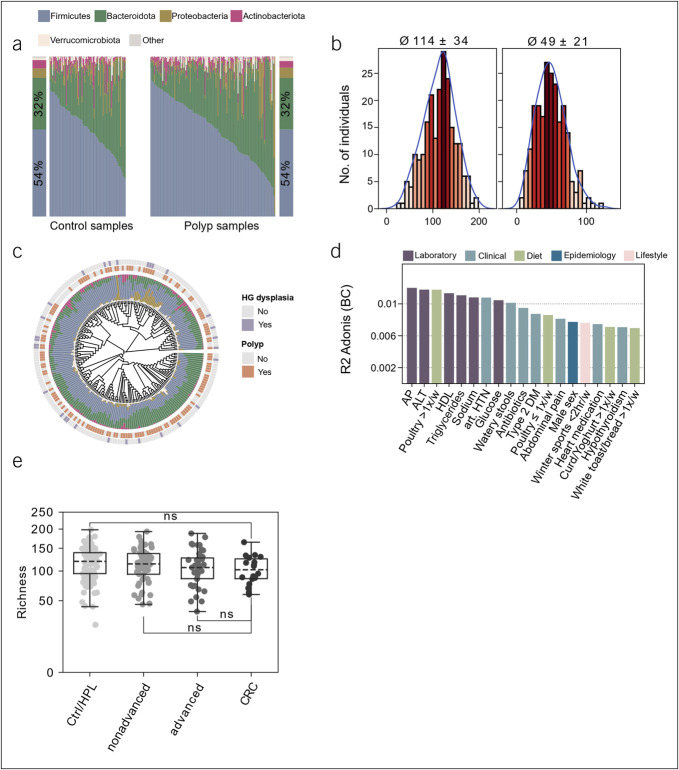
Results: We observed that elevated serum alkaline phosphatase (AP) levels were significantly associated with the presence of high-grade dysplastic polyps. This association was further seen for patients with CRC. Thereby, AP correlated with other parameters of liver function. We did not observe significant changes in the gut microbiota between patients with CP and their respective controls. However, a trend toward a lower alpha-diversity was seen in patients with CRC. Interestingly, AP was identified as a possible clinical effect modifier of stool sample beta diversity.
Discussion: We show for the first time an increased AP in premalignant CP. Furthermore, AP showed a significant influence on the microbial composition of the intestine. Relatively elevated liver enzymes, especially AP, may contribute to the detection of precancerous dysplastic or neoplastic changes in colorectal lesions. The association between elevated AP, premalignant CP, and the microbiome merits further study.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Conflict of interest statement
Figures
References
-
- Morgan E, Arnold M, Gini A, et al. . Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from GLOBOCAN. Gut 2023;72(2):338–44. - PubMed
-
- Lieberman DA, Rex DK, Winawer SJ, et al. . Guidelines for colonoscopy surveillance after screening and polypectomy: A consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2012;143(3):844–57. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
