

Incidence of Respiratory Syncytial Virus-Associated Lower Respiratory Tract Illness in Infants in Low- and Middle-Income Regions During the Coronavirus Disease 2019 Pandemic
- PMID: 38088983
- PMCID: PMC10715683
- DOI: 10.1093/ofid/ofad553
Incidence of Respiratory Syncytial Virus-Associated Lower Respiratory Tract Illness in Infants in Low- and Middle-Income Regions During the Coronavirus Disease 2019 Pandemic
Abstract
Background: Incidence data of respiratory syncytial virus-associated lower respiratory tract illness (RSV-LRTI) are sparse in low- and middle-income countries (LMICs). We estimated RSV-LRTI incidence rates (IRs) in infants in LMICs using World Health Organization case definitions.
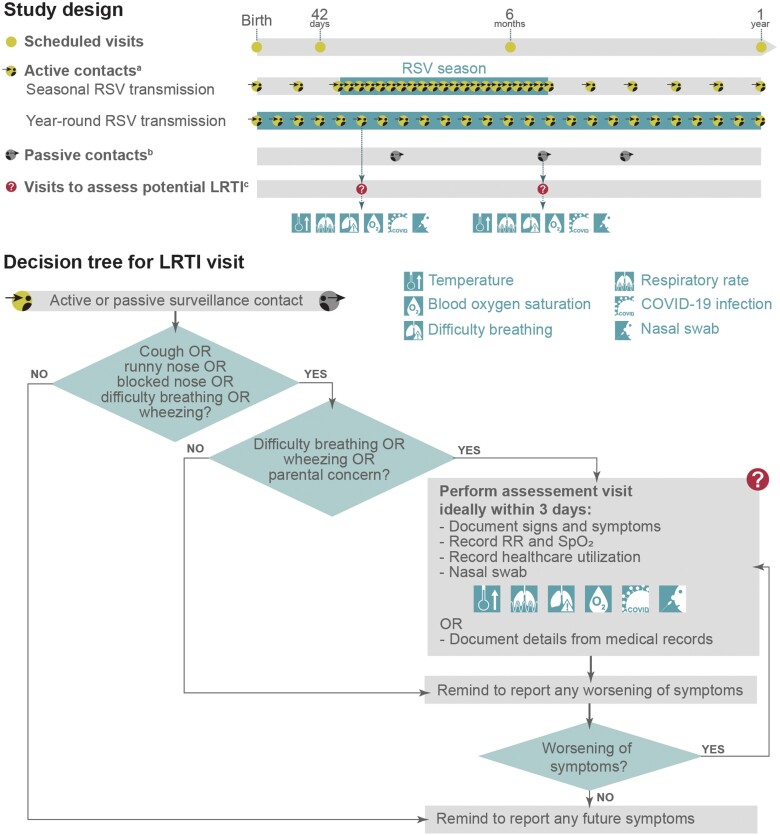
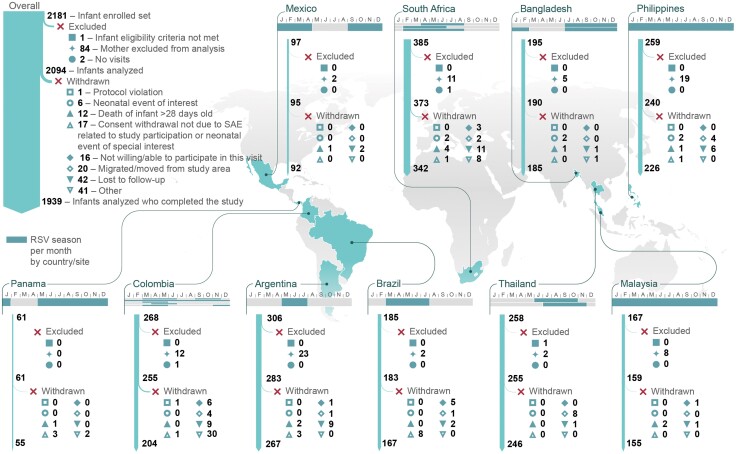
Methods: This prospective cohort study, conducted in 10 LMICs from May 2019 to October 2021 (largely overlapping with the coronavirus disease 2019 [COVID-19] pandemic), followed infants born to women with low-risk pregnancies for 1 year from birth using active and passive surveillance to detect potential LRTIs, and quantitative reverse-transcription polymerase chain reaction on nasal swabs to detect RSV.
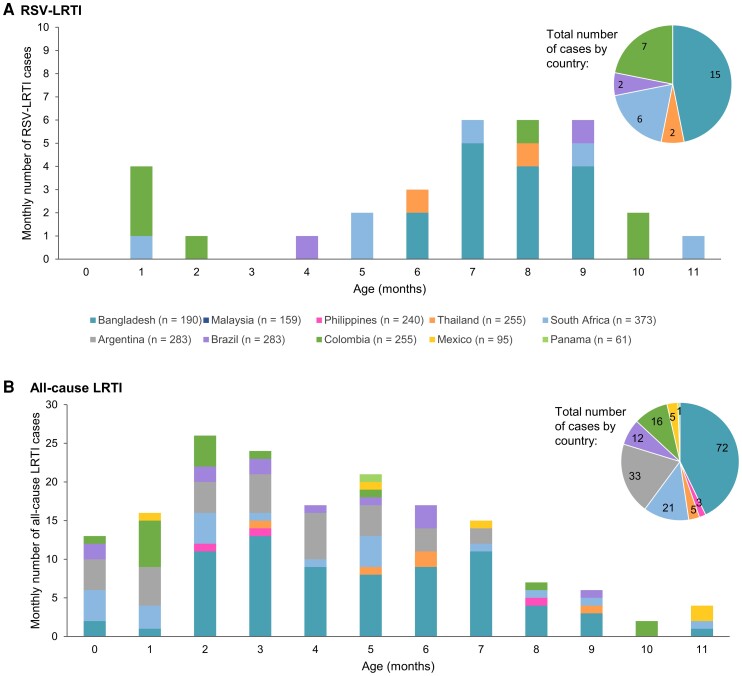
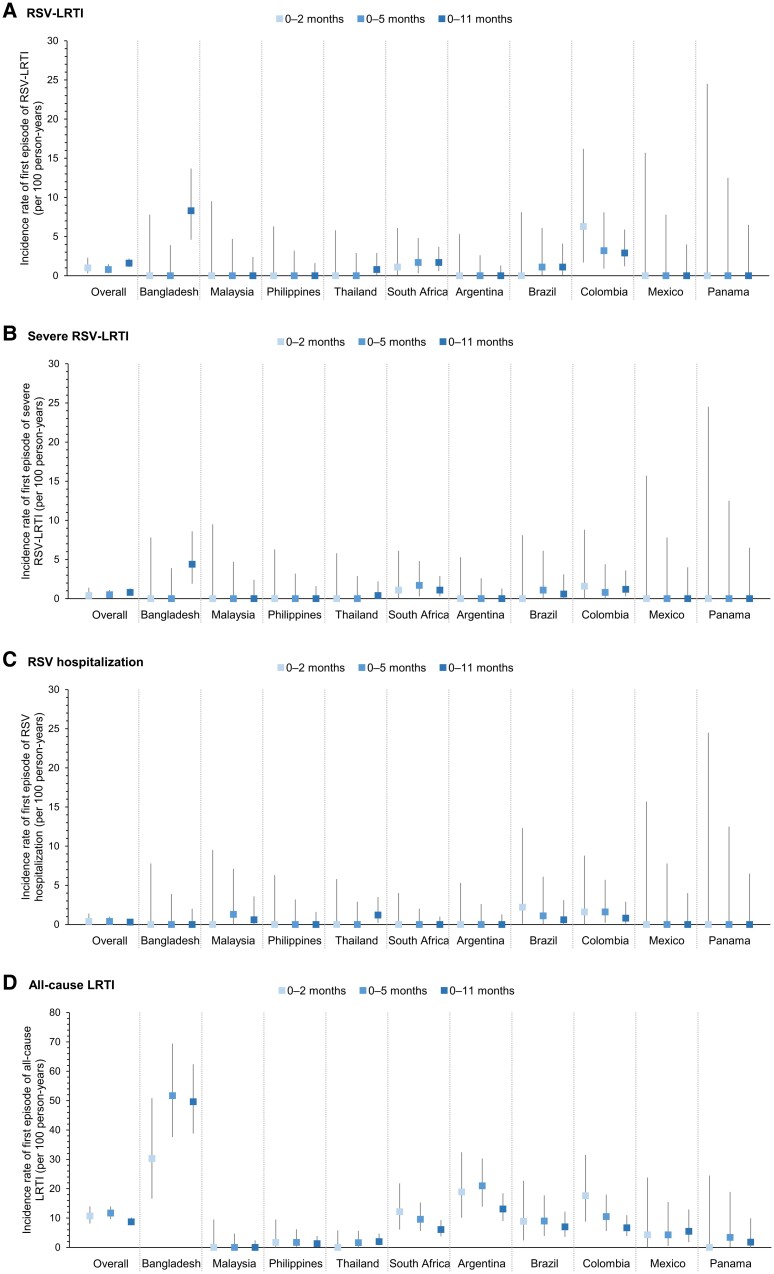
Results: Among 2094 infants, 32 (1.5%) experienced an RSV-LRTI (8 during their first 6 months of life, 24 thereafter). Seventeen (0.8%) infants had severe RSV-LRTI and 168 (8.0%) had all-cause LRTI. IRs (95% confidence intervals [CIs]) of first RSV-LRTI episode were 1.0 (.3-2.3), 0.8 (.3-1.5), and 1.6 (1.1-2.2) per 100 person-years for infants aged 0-2, 0-5, and 0-11 months, respectively. IRs (95% CIs) of the first all-cause LRTI episode were 10.7 (8.1-14.0), 11.7 (9.6-14.0), and 8.7 (7.5-10.2) per 100 person-years, respectively. IRs varied by country (RSV-LRTI: 0.0-8.3, all-cause LRTI: 0.0-49.6 per 100 person-years for 0- to 11-month-olds).
Conclusions: RSV-LRTI IRs in infants in this study were relatively low, likely due to reduced viral circulation caused by COVID-19-related nonpharmaceutical interventions.
Clinical trials registration: NCT03614676.
Keywords: epidemiology; incidence; infants; lower respiratory tract illness; respiratory syncytial virus.
© GSK 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. J. H. K., A. N. T., E. Y., O. H., Y. P., and G. D. S. were employees of GSK when the study was designed, initiated, or conducted. J. H. K., A. N. T., E. Y., O. H., and G. D. S. declare they hold or held shares in GSK as part of their remuneration. A. A. and S. P. work for Keyrus Life Science on behalf of GSK. C. d. C. F. A. received payment from GSK for participation in the study, patient consultations, and ultrasounds. E. L. M. declares research grants from GSK, SP, Janssen, MSD, and the World Health Organization. T. P. received research grants from GSK through her institution. C. M. F. L. received consulting fees and payment for travel expenses for an investigator meeting from GSK and reports payment by GSK to Clinical Research Malaysia. A. V. S. declares research grant from GSK and grants or contracts from MSD, AstraZeneca, Esperion, Clover Biopharm, and F2G. L. S. declares payments from GSK to her institution as a research site for this study. R. S. reports study management and funding as principal investigator from GSK. J. B. V. M. declares payment received for a speaker's bureau for Wyeth Nutrition and participation as Chair of institutional review board, Chair of the Department of Health Single Joint Ethics review board, Chair of the Philippine Health Research Ethics Network, and member of the Philippine Health Technology Assessment Council. M. M. M. P. declares payment from GSK to her institution as a research site for this study. All other authors report no potential conflicts.
Figures
References
-
- GBD 2016 Lower Respiratory Infections Collaborators . Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis 2018; 18:1191–210. - PMC - PubMed
-
- Obando-Pacheco P, Justicia-Grande AJ, Rivero-Calle I, et al. Respiratory syncytial virus seasonality: a global overview. J Infect Dis 2018; 217:1356–64. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
