

Characteristics of pulmonary infarction in patients with acute pulmonary embolism in China: a single-center retrospective observational study
- PMID: 38090315
- PMCID: PMC10713312
- DOI: 10.21037/jtd-23-944
Characteristics of pulmonary infarction in patients with acute pulmonary embolism in China: a single-center retrospective observational study
Abstract
Background: Pulmonary infarction (PI) is an uncommon complication of pulmonary embolism (PE). The risk factors of PI are still relatively unclear.
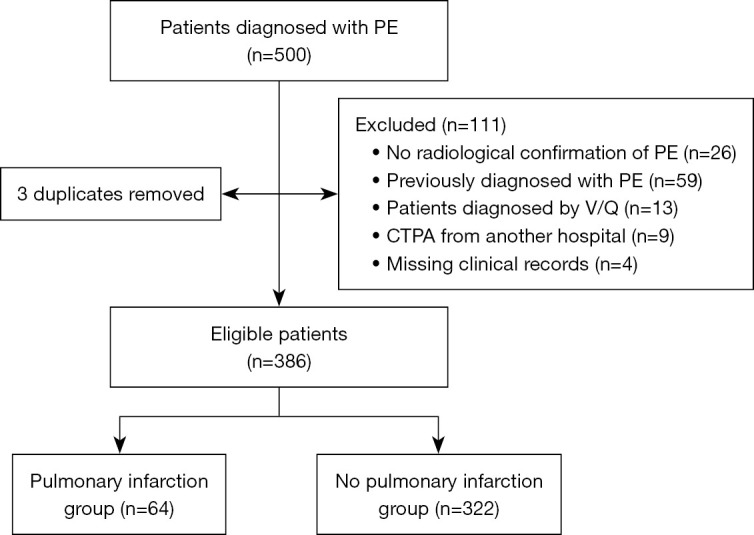
Methods: This was a single-center retrospective review conducted on 500 patients with PE. After applying the inclusion and exclusion criteria, 386 patients diagnosed with PE were enrolled in our study. These patients were then categorized into the PI group (n=64) and the non-PI group (n=322). A comparison was conducted between the two groups regarding the clinical characteristics.
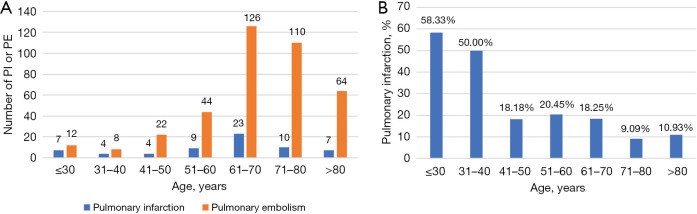
Results: The occurrence of PI secondary to PE was 16.58%. In univariate analysis, recent trauma (21.9% vs. 9.9%, P=0.007), pleuritic chest pain (46.9% vs. 17.4%, P<0.001), hemoptysis (29.7% vs. 2.5%, P<0.001), fever (26.6% vs. 8.1%, P<0.001), lower limb edema/pain (37.5% vs. 14.0%, P<0.001), white blood cell (WBC) counts (37.5% vs. 24.5%, P=0.032), C-reactive protein (CRP) (65.6% vs. 41.3%, P<0.001), and pleural effusion (45.3% vs. 18.6%, P<0.001) were associated with an increased risk of PI. Multivariate analysis demonstrated that age [odds ratio (OR) 0.975, 95% confidence interval (CI): 0.951-0.999, P=0.045], pleuritic chest pain (OR 2.878, 95% CI: 1.424-5.814, P=0.003), hemoptysis (OR 10.592, 95% CI: 3.503-32.030, P<0.001), lower limb edema/pain (OR 2.778, 95% CI: 1.342-5.749, P=0.006) and pleural effusion (OR 3.127, 95% CI: 1.531-6.388, P=0.002) were independent factors of PI due to PE. No significant difference was recorded between the two groups in treatment and mortality.
Conclusions: Young patients were found to be a higher risk of PI. Pleural effusion was found to be a factor for PI. PI should be considered when pleuritic chest pain, hemoptysis, or lower limb edema/pain are present with peripheral opacity.
Keywords: Pulmonary embolism (PE); pulmonary infarction (PI); risk factor.
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-23-944/coif). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous