

Measures of Longitudinal Immune Dysfunction and Risk of AIDS and Non-AIDS Defining Malignancies in Antiretroviral-Treated People With Human Immunodeficiency Virus
- PMID: 38092042
- PMCID: PMC11006099
- DOI: 10.1093/cid/ciad671
Measures of Longitudinal Immune Dysfunction and Risk of AIDS and Non-AIDS Defining Malignancies in Antiretroviral-Treated People With Human Immunodeficiency Virus
Abstract
Background: Human immunodeficiency virus (HIV) infection leads to chronic immune activation/inflammation that can persist in virally suppressed persons on fully active antiretroviral therapy (ART) and increase risk of malignancies. The prognostic role of low CD4:CD8 ratio and elevated CD8 cell counts on the risk of cancer remains unclear.
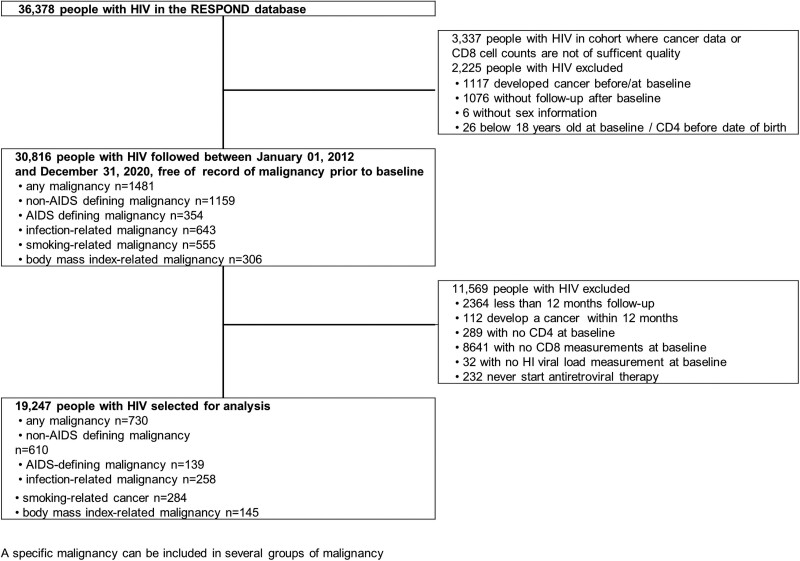
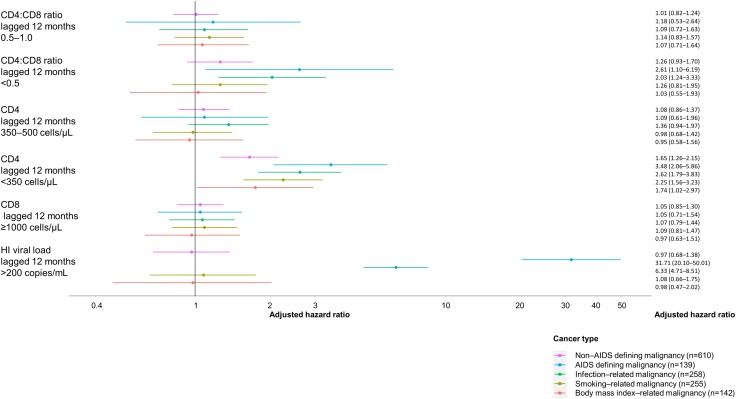
Methods: We investigated the association of CD4:CD8 ratio on the hazard of non-AIDS defining malignancy (NADM), AIDS-defining malignancy (ADM) and most frequent group of cancers in ART-treated people with HIV (PWH) with a CD4 and CD8 cell counts and viral load measurements at baseline. We developed Cox proportional hazard models with adjustment for known confounders of cancer risk and time-dependent cumulative and lagged exposures of CD4:CD8 ratio to account for time-evolving risk factors and avoid reverse causality.
Results: CD4:CD8 ratios below 0.5, compared to above 1.0, were independently associated with a 12-month time-lagged higher risk of ADM and infection-related malignancies (adjusted hazard ratio 2.61 [95% confidence interval {CI }1.10-6.19] and 2.03 [95% CI 1.24-3.33], respectively). CD4 cell counts below 350 cells/μL were associated with an increased risk of NADMs and ADMs, as did infection, smoking, and body mass index-related malignancies.
Conclusions: In ART-treated PWH low CD4:CD8 ratios were associated with ADM and infection-related cancers independently from CD4 and CD8 cell counts and may alert clinicians for cancer screening and prevention of NADM.
Keywords: CD4:CD8 ratio; HIV infection; antiretroviral therapy; malignancy; observational study.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. A. Ma. is full-time employee at Gilead Sciences and owns stock. A. Mo. has received travel support, lecture and consultancy fees from Gilead, ViiV Healthcare, and Eiland and Bonnin, all outside the submitted work. A. E. has received consulting fees and honoraria for lectures and presentations from Roche. C. M. has received honoraria for lectures and presentations from Gilead, ViiV Healthcare, MSD, and travel support from Gilead and a research grant to institution from Gilead. J. J. V. has received honoraria for lectures and presentations from Merck/MSD, Gilead, Pfizer, Astellas Pharma, Basilea, Deutsches Zentrum für Infektionsforschung, Uniklinik Freiburg/Kongress und Kommunikation, Akademie für Infektionsmedizin, University Manchester, Deutsche Gesellschaft für lnfektiologie, Ärztekammer Nordrhein, Uniklinik Aachen, Back Bay Strategies, Deutsche Gesellschaft für Innere Medizin, Shionogi, Molecular Health, Netzwerk Universitätsmedizin, Janssen, NordForsk, Biontech, APOGEPHA, and is part of the data safety monitoring board of APOGEPHA Arznemittel, Biontech, Merck/MSD, Gilead, and Pfizer; and reports research funding from Merck/MSD; Gilead, Pfizer, Astellas Pharma, Basilea, German Centre for Infection Research (DZIF), German Federal Ministry of Education and Research (BMBF), Deutsches Zetrum für Luft und Raumfahrt (DLR), University of Bristol, Rigshospitalet Kopenhagen. A. C. has received honoraria for lectures and presentation and meetings attendance support from Gilead, ViiV Healthcare, MSD, Janssen-Cilag and is part of the advisory board of Gilead, ViiV Healthcare, MSD and Janssen-Cilag. J. B. has received consulting fees and honoraria for lectures and presentations from ViiV Healthcare, Merck, Gilead, Janssen, Pfizer, and Theratechnology, and honoraria from NovoNordisk and AtraZeneca. S. W. is part of the advisory board of ViiV Healthcare and reports grants or contracts paid to institution from RESPOND. R.M. has received consultancy fees from Tamro Baltics, honoraria honoraria for lectures and presentations from MSD, KRKA, Tamro Baltics, AbbVie and Eurovaistine, payment for expert testimony from Tamor Baltic and meeting attendance support from AbbVie, MSD, Johnson&Johnson, and Swixx BioPharma; and reports unpaid roles as Board member of Lithuanian Infectious Diseases Society and as Scientific committee member of EuroSIDA; and the following grants or contracts unrelated to this work: EuroSIDA/Respond, observational cohort study; WEEPI 1.1, WEEPI 1.2 (Western-Eastern European partnership Initiative on HIV, viral hepatitis and TB). J. T. is a member of the European AIDS Treatment Group, a community organization that receives funding not related to this publication from ViiV Healthcare, Gilead Sciences, MSD, Janssen, Orasure Technologies, European Union (author was paid for project work), Innovative Medicines Initiative, FIND Diagnosis, received consulting fees/honoraria from The Global Fund, UNAIDS, Pan American Health Organization, Frontline AIDS, the Barcelona Institute for Global Health. H. G. is an employee of ViiV healthcare and shareholder of GSK. A.Ma. is an employee and shareholder of Gilead Sciences California. H. C. B. has received in the 36 months prior to the submission of this manuscript one grant from Gilead that was not related to this project. HCB has served as the president of the “association contre le HIV et autres infections transmissibles.” In this role he has received support for the Swiss HIV Cohort Study from ViiV Healthcare, Gilead, BMS, and MSD. M. L. reports paid participation on DSMB with Certa Therapeutics. F.W. reports participation in advisory board for ViiV Healthcare. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Morlat P, Roussillon C, Henard S, et al. Causes of death among HIV-infected patients in France in 2010 (national survey): trends since 2000. AIDS 2014; 28:1181–91. - PubMed
-
- Clifford GM, Polesel J, Rickenbach M, et al. Cancer risk in the Swiss HIV cohort study: associations with immunodeficiency, smoking, and highly active antiretroviral therapy. J Natl Cancer Inst 2005; 97:425–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
