

Effect of transcutaneous electrical acupoint stimulation on remifentanil dosage during craniotomy aneurysm clipping: a prospective, randomized controlled study
- PMID: 38093254
- PMCID: PMC10717748
- DOI: 10.1186/s12906-023-04297-x
Effect of transcutaneous electrical acupoint stimulation on remifentanil dosage during craniotomy aneurysm clipping: a prospective, randomized controlled study
Abstract
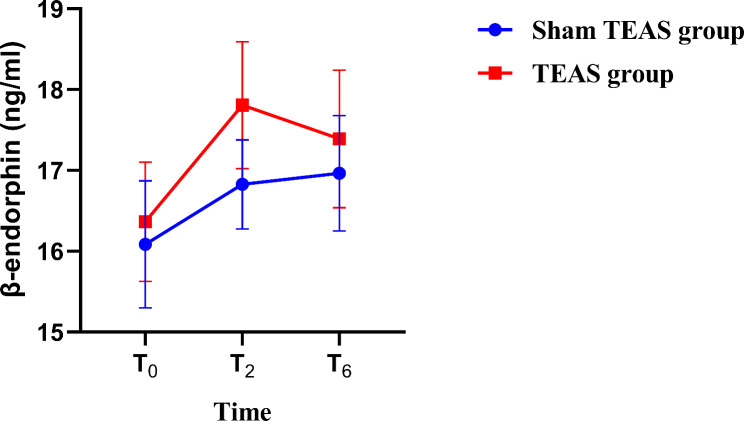
Background: Craniotomy aneurysm clipping is one of the main treatments for intracranial aneurysm (IA). Endotracheal intubation and intraoperative operation may induce dramatic hemodynamic fluctuations and increase the risk of aneurysm rupture. Intraoperative high-dose opioid use is the main measure to reduce the intraoperative stress response, but it increases the incidence of complications such as postoperative vomiting and delayed awakening. Transcutaneous electrical acupoint stimulation (TEAS) stimulates β-endorphin expression levels and reduces opioid requirements. In this study, we aimed to assess the effects of TEAS on remifentanil dosage and oxidative stress (OS) in craniotomy aneurysm clipping.
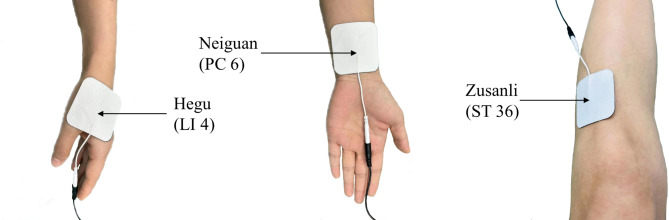
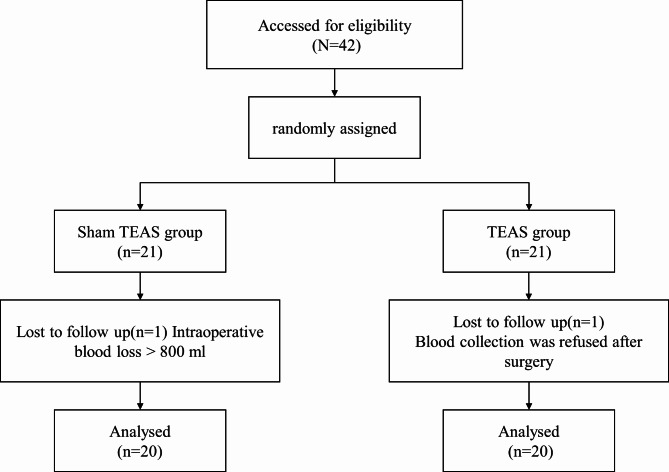
Method: Forty-two patients with craniotomy aneurysm clipping were randomized into two groups: the TEAS group (T group) and the sham TEAS group (S group). "Hegu" (LI4), "Neiguan" (PC6) and "Zusanli" points (ST36) were selected, and a "HANS" percutaneous acupoint electrical stimulator was used for intervention 30 min before anesthesia induction until the end of the operation. The primary outcome was intraoperative remifentanil dosage. The secondary outcomes were intraoperative propofol dosage, mean arterial pressure (MAP) and heart rate (HR) 5 min before the TEAS intervention (T0), 5 min before head holder pinning (T1), immediately after pinning (T2), 5 min before craniotomy (T3), immediately after craniotomy (T4), at craniotomy (T5), and at the end of surgery (T6), as well as serum β-endorphin levels at T1, T2 and T6 and neuron-specific enolase (NSE), S100β, superoxide dismutase (SOD) and malondialdehyde (MDA) levels at T1, T2 and 24 h after surgery (T7).
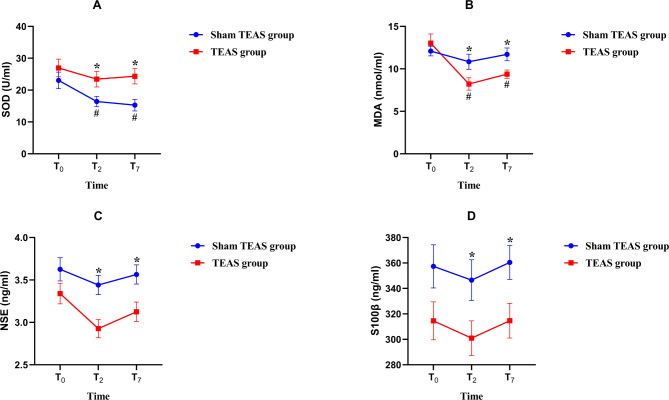
Results: The dosage of remifentanil in the T group was reduced compared to that in the S group (P < 0.05). At T2, T4 and T5, the MAP and HR in the T group were lower than those in the S group (P < 0.05). At T2 and T7, the levels of NSE, S100β and MDA in group T were lower than those in group S (P < 0.05), while the SOD levels in group T were higher than those in group S (P < 0.05).
Conclusions: The use of TEAS can reduce the dosage of remifentanil and reduce hemodynamic fluctuations during craniotomy aneurysm clipping. It reduces the occurrence of OS and central nervous system damage during surgery and has a certain brain protective effect.
Trial registration: ChiCTR2100052353. https://www.chictr.org.cn/about.html .
Keywords: Brain injury; Craniotomy Aneurysm clipping; Oxidative stress; Remifentanil; Transcutaneous electrical acupoint stimulation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
- 2019A091/Jiangxi Provincial Administration of Traditional Chinese Medicine
- 2019A091/Jiangxi Provincial Administration of Traditional Chinese Medicine
- 2019A091/Jiangxi Provincial Administration of Traditional Chinese Medicine
- 2019A091/Jiangxi Provincial Administration of Traditional Chinese Medicine
- 2019A091/Jiangxi Provincial Administration of Traditional Chinese Medicine
LinkOut - more resources
Full Text Sources
Medical
