

Negative Impact of TET2 Mutations on Long-Term Survival After Transcatheter Aortic Valve Replacement
- PMID: 38093739
- PMCID: PMC10714177
- DOI: 10.1016/j.jacbts.2023.04.010
Negative Impact of TET2 Mutations on Long-Term Survival After Transcatheter Aortic Valve Replacement
Abstract
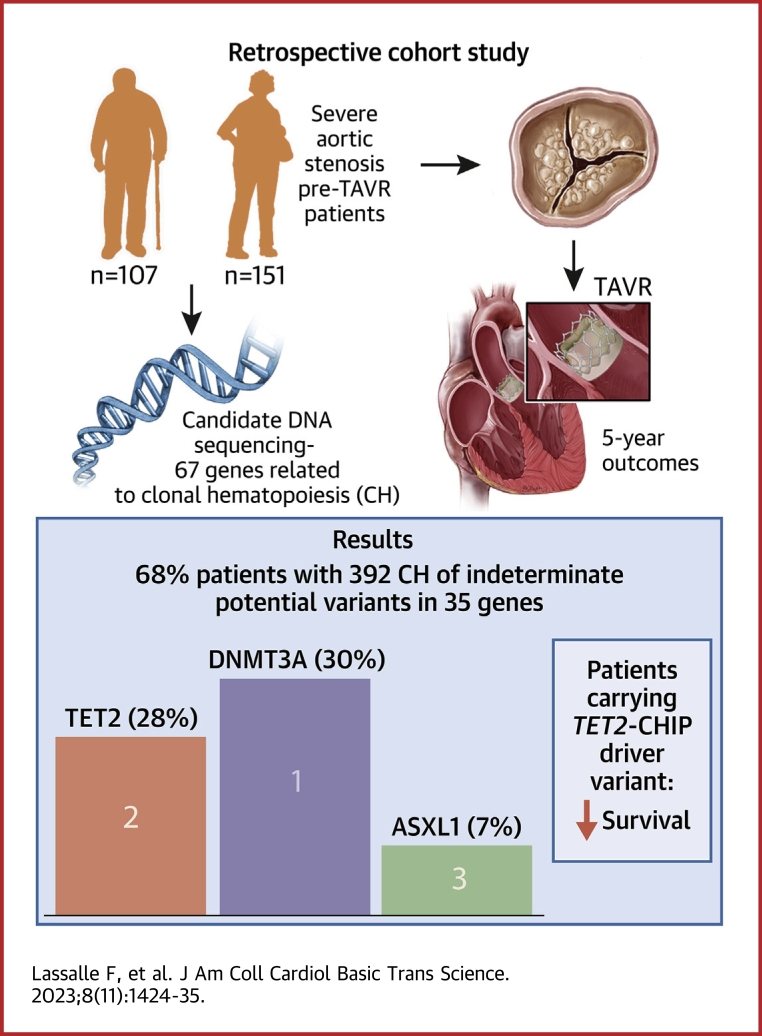
Clonal hematopoiesis of indeterminate potential (CHIP) is considered as being a novel age-related risk factor for cardiovascular diseases. By capture-sequencing of a 67-gene panel, we established a large spectrum of CHIP in 258 patients with aortic valve stenosis undergoing transcatheter aortic valve replacement (TAVR) and assessed their association with long-term survival after TAVR. One or several CHIP variants in 35 genes were identified in 68% of the cohort, DNMT3A and TET2 being the 2 most frequently mutated genes. Patients carrying a TET2-CHIP-driver variant with low variant allele frequency (2%-10%) had a significant decrease in overall survival 5 years after TAVR.
Keywords: aortic valve stenosis; clonal hematopoiesis; survival; transcatheter aortic valve replacement.
© 2023 The Authors.
Conflict of interest statement
Dr Staels is supported by grants from the Fondation Leducq convention 6CVD01 “Defining and targeting epigenetic pathways in monocytes and macrophages that contribute to cardiovascular disease,” the European Genomic Institute for Diabetes (EGID, ANR-10-LABX-0046), and is a recipient of an Advanced ERC Grant (694717). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.PerspectivesCOMPETENCY IN MEDICAL KNOWLEDGE: AVS is an elderly pathology mediated by inflammation. CHIP has been recently described as a novel age-related risk factor for cardiovascular diseases. This study describes in a cohort of 258 patients a large profile and a high prevalence of CHIP-driver genes in AVS. Moreover, patients carrying TET2 mutations with low VAF (2%-10%) have a decreased overall survival at 5 years after TAVR. These findings contribute to the understanding of the pathogenesis of AVS and might help decision making in the management of patients with AVS undergoing TAVR. TRANSLATIONAL OUTLOOK: Additional functional studies in relevant preclinical models are still needed to unravel the exact mechanisms by which CHIP-driver variants contribute to AVS and impact the clinical prognosis after TAVR, especially in TET2. Our findings need to be validated in larger studies of consecutive patients before being used for decision making in the management of patients with severe AVS undergoing TAVR. There are a number of studies that showed that TET2 deficiency in murine models leads to an enhanced inflammation, particularly via IL-1β and NLRP3 inflammasome. Our study emphasizes the fact that IL-1β and the inflammasome could be novel therapeutic targets in AVS and for the improvement of survival after TAVR for patients who are carrying TET2 somatic variants.
Figures





References
-
- Popma J.J., Deeb G.M., Yakubov S.J., et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. 2019;380(18):1706–1715. - PubMed
-
- Otto C.M., Nishimura R.A., Bonow R.O., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease. J Am Coll Cardiol. 2021;77(4):450–500. - PubMed
-
- Vahanian A., Beyersdorf F., Praz F., et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561–632. - PubMed
LinkOut - more resources
Full Text Sources
