

Successful endovascular management of coral reef aortic occlusion
- PMID: 38093924
- PMCID: PMC10713881
- DOI: 10.1007/s12055-023-01656-8
Successful endovascular management of coral reef aortic occlusion
Abstract
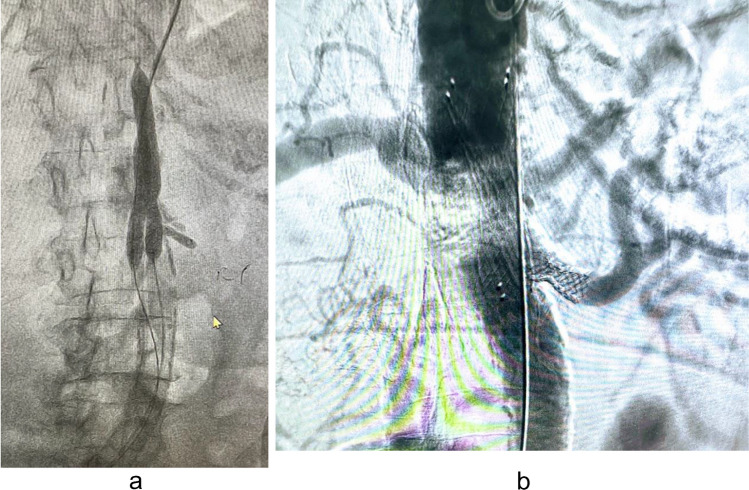
Transaortic thromboendarterectomy and bypass have been the conventional treatment for coral reef aortic occlusions but are associated with significant mortality, morbidity and reintervention rate since these patients often present with heart failure, uncontrolled hypertension and renal dysfunction. Endovascular treatment has not become popular because of fear of aortic rupture and visceral ischemia. We present our experience with endovascular management of 10 patients with coral reef aorta. Uncontrolled hypertension, chronic renal disease, disabling claudication, and critical limb ischemia with tissue loss were the presenting symptoms. Seven patients had infrarenal aortic occlusion, and 3 had occlusion at renal and suprarenal aorta. Eight had involvement of the visceral vessels and 3 had renal artery stenosis. Common iliac, femoral and subclavian were the other arteries involved. All procedures were done under local anaesthesia. Aortic stenting was done in 7 and aortoiliac stent in 3. Two had covered stents and the rest had bare metal stents. Two had renal artery stenting. In 2 patients with suprarenal aortic occlusion, intravascular lithotripsy was used prior to aortic stenting. We achieved technical success in all patients with control of blood pressure and increase in Ankle Brachial Index (ABI). One patient died due to acute coronary event 2 months later.
Keywords: Aortic calcification; Aortic stenting; Coral reef aorta; Visceral protection, intravascular lithotripsy.
© Indian Association of Cardiovascular-Thoracic Surgeons 2023.
Conflict of interest statement
Conflict of interestThe authors declare no competing interests.
Figures




References
-
- Qvarfordt PG, Reilly LM, Sedwitz MM, Ehrenfeld WK, Stoney RJ. “Coral reef” atherosclerosis of the suprarenal aorta: a unique clinical entity. J Vasc Surg. 1984;1:903–909. - PubMed
-
- Minnee RC, Idu MM, Balm R. Coral reef aorta: case reports and review of the literature. Ejves Extra. 2005;9:39–43. doi: 10.1016/j.ejvsextra.2005.02.006. - DOI
LinkOut - more resources
Full Text Sources