

Pharmacokinetics and Proposed Dosing of Levetiracetam in Children With Obesity
- PMID: 38094673
- PMCID: PMC10715382
- DOI: 10.5863/1551-6776-28.8.693
Pharmacokinetics and Proposed Dosing of Levetiracetam in Children With Obesity
Abstract
Objective: Characterize levetiracetam pharmacokinetics (PK) in children with obesity to inform dosing.
Methods: Children 2 to <21 years old receiving standard of care oral levetiracetam across two opportunistic studies provided blood samples. Levetiracetam plasma PK data were analyzed with a nonlinear mixed-effects modeling approach. Indirect measures for body size and covariates were tested for model inclusion. Individual empirical Bayesian estimates using the final model parameters were compared by obesity status. Monte Carlo simulation using total body weight was performed in children with normal estimated glomerular filtration rate to identify dosing for children with obesity that resulted in comparable exposures to normal weight adults and children after receiving label dosing.
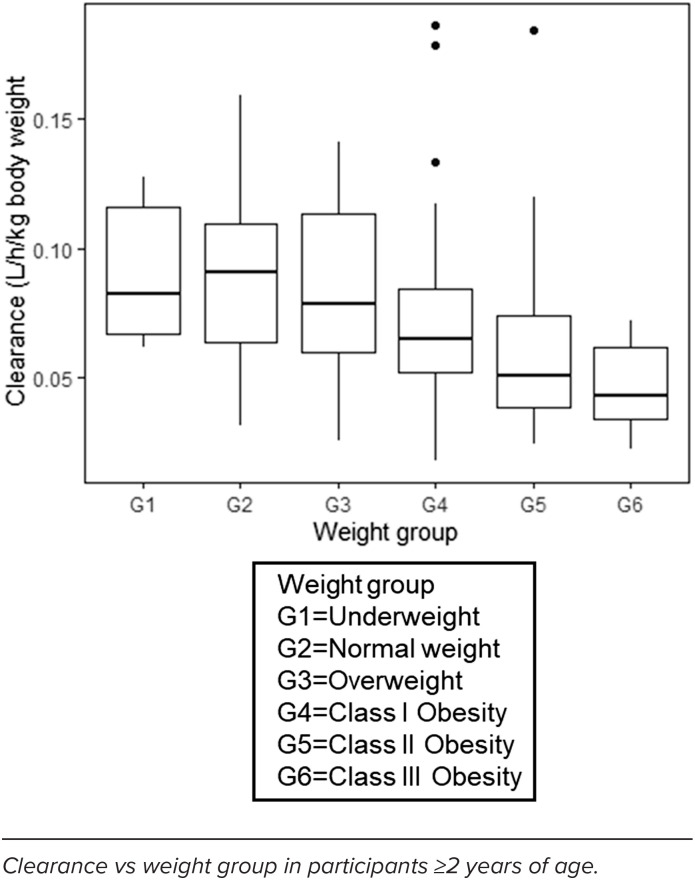
Results: The population PK model was developed from 341 plasma concentrations from 169 children. A 1-compartment model best fit the data with fat-free mass as a significant covariate. Compared with children with normal weight, children with obesity had significantly lower body weight-normalized clearance (median [range], 4.77 [1.49-10.44] and 3.71 [0.86-13.55] L/h/70 kg, respectively). After label dosing with the oral formulation in children with obesity 4 to <16 years old, maximum and minimum steady-state concentrations were higher (25% and 41%, respectively [oral solution] and 27% and 19%, respectively [tablet]) compared with children with normal weight. Comparable exposures between children with and without obesity were achieved with weight-tiered dosing regimens of <75 kg or ≥75 kg.
Conclusions: Weight-tiered dosing for levetiracetam oral solution and tablets for children with obesity 4 to <16 years old results in more comparable exposures to children of normal weight.
Keywords: Keppra; children; levetiracetam; obesity; pharmacokinetics.
Copyright. Pediatric Pharmacy Association. All rights reserved. For permissions, email: membership@pediatricpharmacy.org.
Figures



References
-
- Keppra (levetiracetam) [package insert] Smyrna, GA: UCB; Oct, 2019.
-
- Centers for Disease Control and Prevention (CDC) Defining childhood weight status. Updated December . 2021;3 Accessed April 21, 2022. https://www.cdc.gov/obesity/childhood/defining.html.
-
- Fryar CD CM, Afful J. Prevalence of overweight, obesity, and severe obesity among children and adolescents aged 2–19 years: United States, 1963–1965 through 2017–2018. National Center for Health Statistics (NCHS) Health E-Stats. Published 2020. Updated January 29, 2021. Accessed April 21, 2022. https://www.cdc.gov/nchs/data/hestat/obesity-child-17-18/obesity-child.h....
-
- Mulla H, Johnson TN. Dosing dilemmas in obese children. Arch Dis Child Educ Pract Ed . 2010;95(4):112–117. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources