

A Modified Technique for All-Inside Anterior Cruciate Ligament Reconstruction (ACLR): True Femoral Socket
- PMID: 38094943
- PMCID: PMC10714371
- DOI: 10.1016/j.eats.2023.07.025
A Modified Technique for All-Inside Anterior Cruciate Ligament Reconstruction (ACLR): True Femoral Socket
Abstract
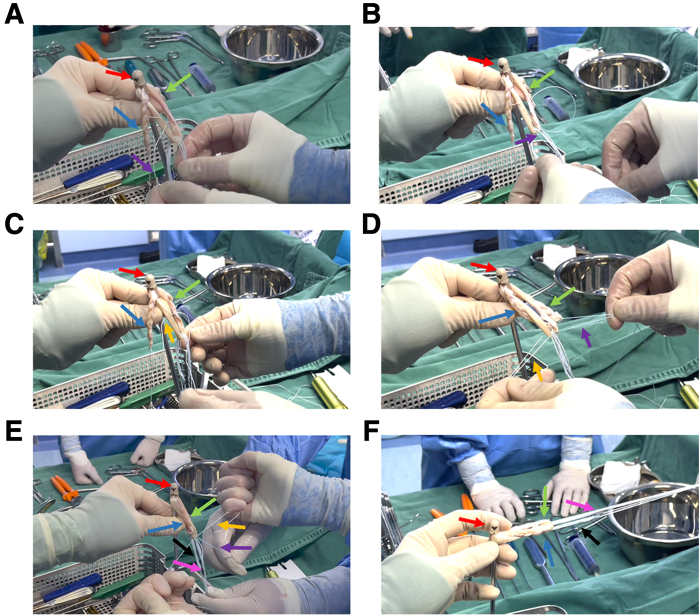
Anterior cruciate ligament reconstruction (ACLR) performed via arthroscopy is the primary treatment for anterior cruciate ligament injury. In traditional ACLR, the surgeon must create bone tunnels in both the femur and tibia, which increases the risk of bleeding and pain. The advent of all-inside technology has introduced the concept of bone sockets. However, the femoral socket created by the traditional all-inside technique is not a true femoral socket since the tunnel ends are still connected to achieve suspensory fixation. We are dedicated to achieving a true femoral socket in the all-inside ACLR technique. The AperFix Implant fixation system offers the potential for a genuine femoral socket by securely holding the ligaments in place through compression fixation. In this report, we present an all-inside ACLR using the AperFix Implant fixation system, which allows for a single exit of the femur side tunnel. This technique effectively reduces "windshield wiper" effect, "bungee cord" effect, as well as surgical time and minimizes the risk of bleeding, pain, and local microfractures.
© 2023 The Authors.
Figures







References
-
- Khan I., Ullah S., Khattak S.K., Khan Z., Ahmad I., Khan A. Functional outcome of arthroscopic anterior cruciate ligament reconstruction using hamstring autograft with fixation using Endobutton at femoral end and bioabsorbable screw at tibial end. Mymensingh Med J. 2022;31:1142–1147. - PubMed
-
- Zhu J., Marshall B., Tang X., Linde M.A., Fu F.H., Smolinski P. ACL graft with extra-cortical fixation rotates around the femoral tunnel aperture during knee flexion. Knee Surg Sports Traumatol Arthrosc. 2022;30:116–123. - PubMed
-
- Lin R., Zhong Q., Wu X., Cui L., Huang R., Deng Q., et al. Randomized controlled trial of all-inside and standard single-bundle anterior cruciate ligament reconstruction with functional, MRI-based graft maturity and patient-reported outcome measures. BMC Musculoskel Disord. 2022;23:289. - PMC - PubMed
-
- Lin T.Y., Chung C.C., Chen W.C., Su C.W., Fang H.W., Lu Y.C. Complications following all-inside anterior cruciate ligament reconstruction. Int Orthop. 2022;46:2569–2576. - PubMed
LinkOut - more resources
Full Text Sources
