

Early kinetics of C reactive protein for cancer-agnostic prediction of therapy response and mortality in patients treated with immune checkpoint inhibitors: a multicenter cohort study
- PMID: 38097343
- PMCID: PMC10729183
- DOI: 10.1136/jitc-2023-007765
Early kinetics of C reactive protein for cancer-agnostic prediction of therapy response and mortality in patients treated with immune checkpoint inhibitors: a multicenter cohort study
Abstract
Background: C reactive protein (CRP) kinetics have recently been suggested as predictive biomarkers for the efficacy of immune checkpoint inhibitor (ICI) therapy in selected cancer types. The aim of this study was to characterize early CRP kinetics as a tumor-agnostic biomarker for ICI treatment outcomes.
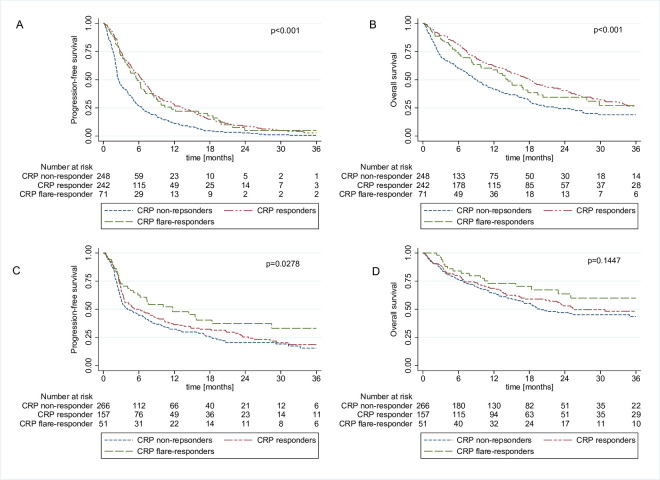
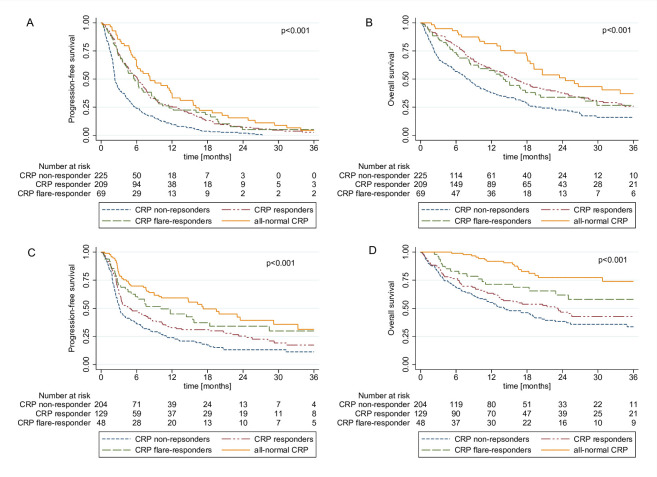
Methods: In this multicenter retrospective cohort study, two independent cohorts of patients with various cancer types undergoing palliative ICI treatment at Austrian academic centers served as the discovery (n=562) and validation cohort (n=474). Four different patterns of CRP kinetics in the first 3 months of ICI therapy were defined (CRP-flare responders, CRP-responders, CRP non-responders, patients with all-normal CRP). Objective response rate (ORR), progression-free survival (PFS) and overall survival (OS) were defined as coprimary endpoints. Univariable and multivariable logistic regression, landmark analysis and Cox regression including CRP kinetics as time-dependent variable were performed.
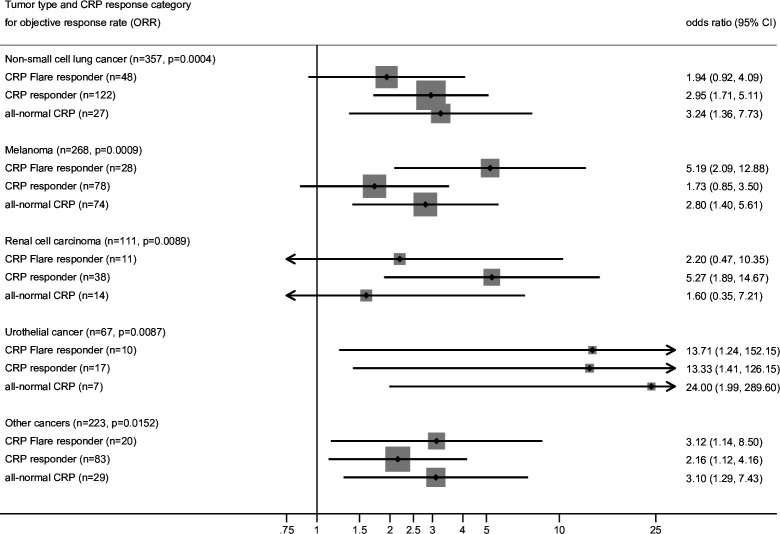
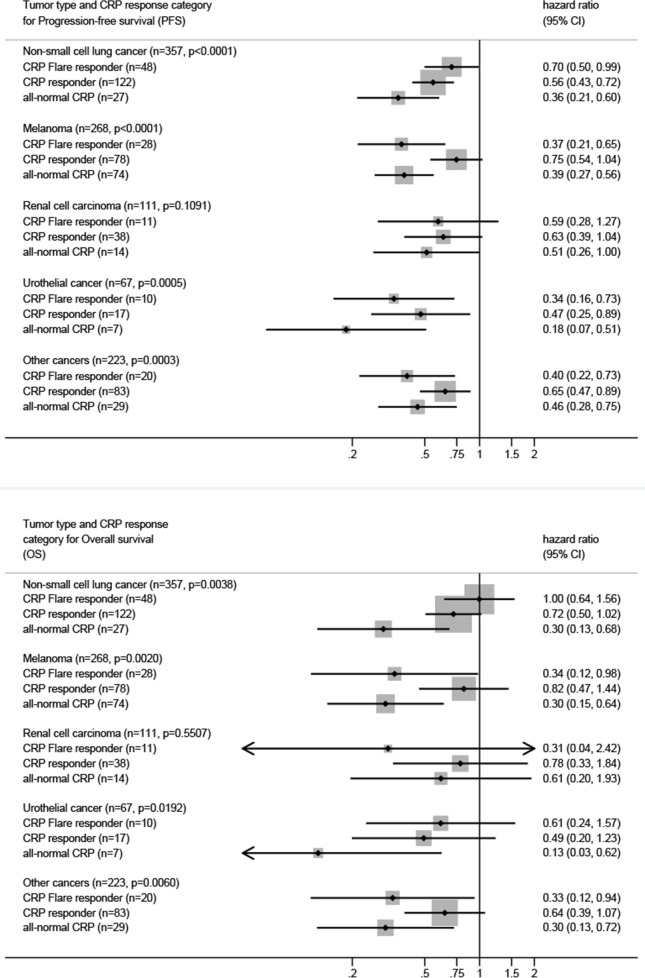
Results: The ORR in patients with all-normal CRP, CRP responders, CRP flare-responders and CRP non-responders was 41%, 38%, 31% and 12%, respectively. The median OS and PFS estimates were 24.5 months (95% CI 18.5 to not reached) and 8.2 months (95% CI 5.9 to 12.0) in patients with all-normal CRP, 16.1 months (95% CI 12.6 to 19-8) and 6.1 months (95% CI 4.9 to 7.2) in CRP-responders, 14.0 months (95% CI 8.5 to 19.4) and 5.7 months (95% CI 4.1 to 8.5) in CRP flare-responders and 8.1 months (95% CI 5.8 to 9.9) and 2.3 months (95% CI 2.2 to 2.8) in CRP non-responders (log-rank p for PFS and OS<0.001). These findings prevailed in multivariable analysis and could be fully confirmed in our validation cohort. Pooled subgroup analysis suggested a consistent predictive significance of early CRP kinetics for treatment efficacy and outcome independent of cancer type.
Conclusion: Early CRP kinetics represent a tumor-agnostic predictor for treatment response, progression risk and mortality in patients with cancer undergoing ICI therapy.
Keywords: Biomarkers, Tumor; Immune Checkpoint Inhibitors.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DAB has received travel/congress support from EISAI, Lilly, Bristol-Myers Squibb, MSD; honoraria for consulting or advisory boards from Roche, EISAI, MSD; honoraria for lectures from Ipsen unrelated to the submitted work. FM received has received honoraria for advisory boards from Servier and Bristol-Myers Squibb. LK has received honoraria for travel/congress support and consulting/advisory roles from Bristol Myers Squibb (BMS), Merck Sharp & Dome (MSD), Novartis, Pierre Fabre and Sanofi Aventis unrelated to the submitted work. ER stated the following conflicts of interest: Honoraria: Amgen, BMS, Delcath, MSD, Merck, Novartis, Pierre Fabre, Sanofi. Consulting or advisory role: Amgen, BMS, MSD, Merck, Novartis, Pierre Fabre, Sanofi. Speakers’ bureau: Amgen, BMS, MSD, Merck, Novartis, Pierre Fabre, Sanofi. Former Site PI for Medical University of Graz (last three years): Amgen, BMS, Curevac, Incyte, MSD, Merck, Novartis, Pierre Fabre, Roche. To date Site PI for Medical University of Graz: Delcath. Steering Committee: Novartis. Travel reimbursements: Amgen, BMS, MSD, Merck, Novartis, Pierre Fabre, Sanofi. Stock (under US$10,000): Roche. Honorary member of the Austrian Cancer Aid and the Austrian Cancer Aid/StyriaMP (Matthias Preusser) has received honoraria for lectures, consultation or advisory board participation from the following for-profit companies: Bayer, Bristol-Myers Squibb, Novartis, Gerson Lehrman Group (GLG), CMC Contrast, GlaxoSmithKline, Mundipharma, Roche, BMJ Journals, MedMedia, Astra Zeneca, AbbVie, Lilly, Medahead, Daiichi Sankyo, Sanofi, Merck Sharp & Dome, Tocagen, Adastra, Gan & Lee Pharmaceuticals, Servier. MP declares no conflict of interest related to this work. JMR has received honoraria for lectures from BMS and MSD.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous