

Discordance between GCIG CA-125 progression and RECIST progression in the CALYPSO trial of patients with platinum-sensitive recurrent ovarian cancer
- PMID: 38097739
- PMCID: PMC10844635
- DOI: 10.1038/s41416-023-02528-z
Discordance between GCIG CA-125 progression and RECIST progression in the CALYPSO trial of patients with platinum-sensitive recurrent ovarian cancer
Abstract
Background: CA-125 alone is widely used to diagnose progressive disease (PD) in platinum-sensitive recurrent ovarian cancer (PSROC) on chemotherapy. However, there are increasing concerns regarding its accuracy. We assessed concordance between progression defined by CA-125 and RECIST using data from the CALYPSO trial.
Methods: We computed concordance rates for PD by CA-125 and RECIST to determine the positive (PPV) and negative predictive values (NPV).
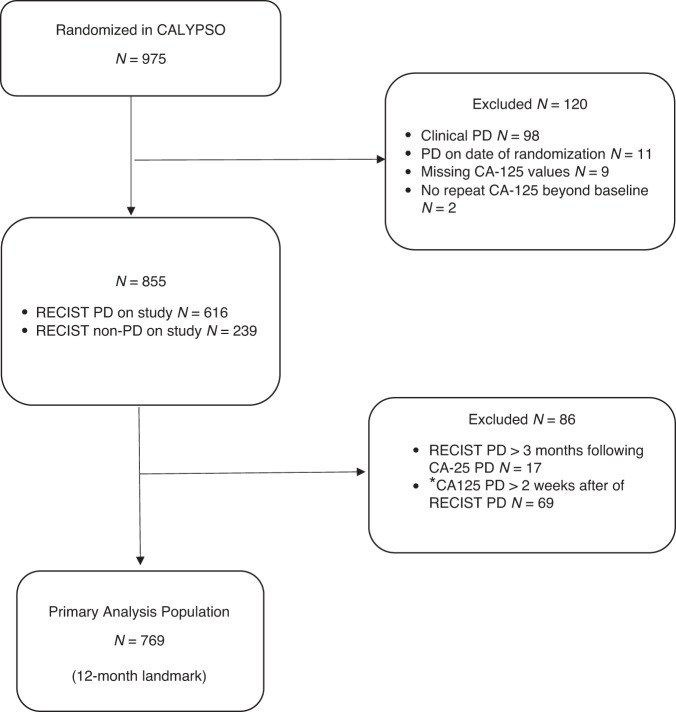
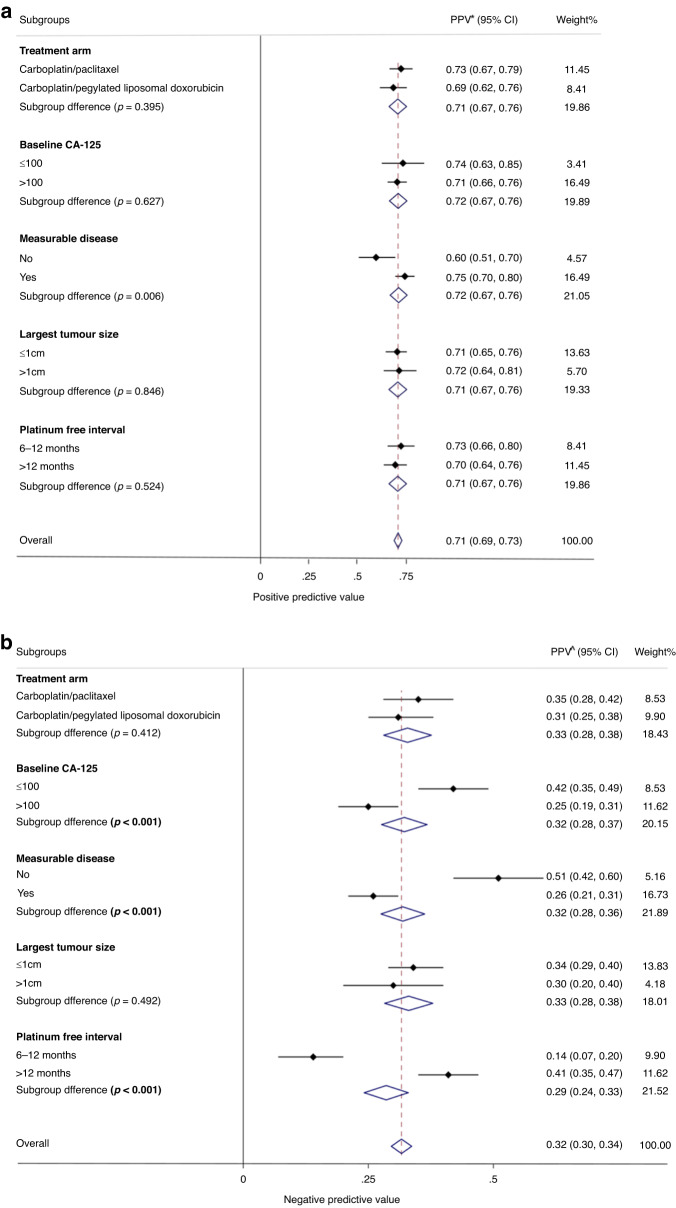
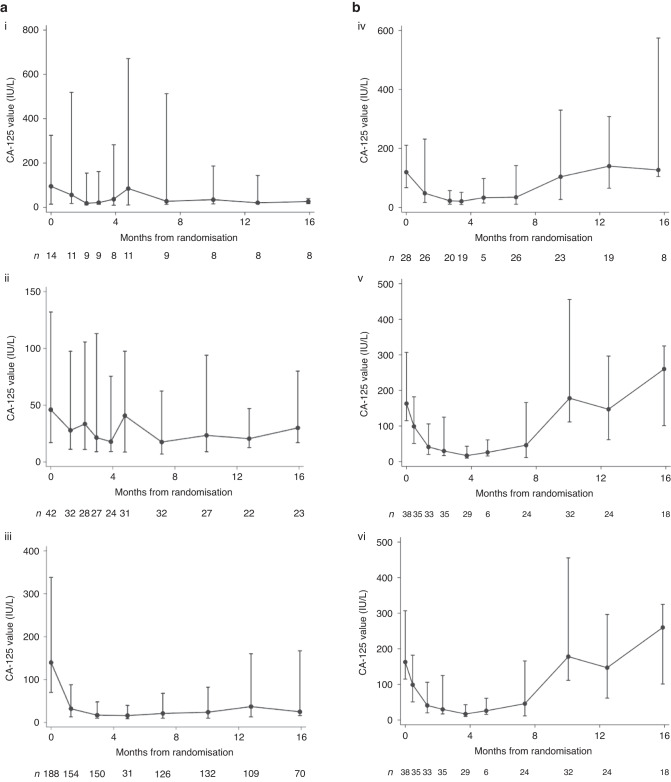
Results: Of 769 (79%) evaluable participants, 387 had CA-125 PD, where only 276 had concordant RECIST PD (PPV 71%, 95% CI 67-76%). For 382 without CA-125 PD, 255 had RECIST PD but 127 did not (NPV 33%, 95% CI 29-38). There were significant differences in NPV according to baseline CA-125 (≤100 vs >100: 42% vs 25%, P < 0.001); non-measurable vs measurable disease (51% vs 26%, P < 0.001); and platinum-free-interval (>12 vs 6-12 months: 41% vs 14%, P < 0.001). We observed falling CA-125 levels in 78% of patients with RECIST PD and CA-125 non-PD.
Conclusion: Approximately 2 in 3 women with PSROC have RECIST PD but not CA-125 PD by GCIG criteria. Monitoring CA-125 levels alone is not reliable for detecting PD. Further research is required to investigate the survival impact of local therapy in radiological detected early asymptomatic PD.
© 2023. Crown.
Conflict of interest statement
D. S. Zebic reports honoraria from Merck. A. Tjokrowidjaja reports research funding (institution) from AZ, support for attending meetings from GSK. K. E. Francis reports funding from BMS, support for attending educational meeting. M. Friedlander reports consulting fees from Novartis, AstraZeneca, MSD, GSK; honoraria from AstraZeneca, GSK, MSD; grants (institution) from AstraZeneca, Novartis, Beigene; participation on a Data Safety Monitoring Board or Advisory Board for AGITG. V. Gebski reports no conflict of interest. A. Lortholary reports participation on Advisory Board for AstraZeneca, MSD Tesaro; honoraria from Clovis Oncology, Roche; congress participation for Novartis, Pfizer, MAD, Lilly, Roche; member of CS3 sein UNICANCER. F. Joly reports participation on Advisory Board for GSK, AstraZeneca, Clovic, Seagen, Janssen, ESAI, Bayer, Viatris, MSD, Ipsen, Amgen, Astellas; honoraria from GSK, Bayer, ESAI, MSD; research funding (personal) from AstraZeneca, GSK; participation member for ASCO, GCIG; congress travel fees from GSK, MSD, ESAI, Ipsen. A. Hasenburg reports honoraria from AstraZeneca, Celgen, GSK, LEO Pharma, MedConcept GmbH, Med update GmbH, Medicultus, Pfizer, Promedicis GmbH, Softconsult, Roche Pharma AG, Streamedup GmbH, Tesaro Bio Germany GmbH; participation on Advisory Board for AstraZeneca, GSK, LEO Pharma, PharmaMar, Promedicis GmbH, Roche Pharma AG, Tesaro Bio Germany GmbH, MSD Sharp&Dohme GmbH. M. Mirza reports participation Data Safety Monitoring Board or Advisory Board for Astra Zeneca, Biocad, GSK, Karyopharm, Merck, Roche, Zailab; honoraria from Astra Zeneca, GSK; research funding (institution) from Apexigen, AstraZeneca, Deciphera (trial chair), GSK, and Ultimovacs; and personal financial interest in Karyopharm (stocks/shares, member of Board of Directors). U. Denison reports no conflict of interest. S. C. Cecere reports honoraria from AstraZeneca, MSD, Pharmamar. A. Ferrero reports honoraria from AstraZeneca, MSD, GlaxoSmithKline, Clovis; participation Data Safety Monitoring Board or Advisory Board for AstraZeneca, MSD. E. Pujade-Lauraine reports honoraria (personal) from AstraZeneca, GSK, Agenus; grants (institution) from AstraZeneca, Merck; participation on Advisory Board or Data Safety Monitoring Board for Incyte, Roche, Pfizer; and is an employee of ARCAGY GINECO research. C.K. Lee reports honoraria from AstraZeneca, Roche, Amgen, GSK, Merck KGA, Novartis, Pfizer, Janssen; grants (institution) from AstraZeneca, Roche, Amgen, Merck KGA; support for attending meetings from AstraZeneca.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
