

Investment case for small and sick newborn care in Tanzania: systematic analyses
- PMID: 38098013
- PMCID: PMC10722687
- DOI: 10.1186/s12887-023-04414-2
Investment case for small and sick newborn care in Tanzania: systematic analyses
Abstract
Background: Small and sick newborn care (SSNC) is critical for national neonatal mortality reduction targets by 2030. Investment cases could inform implementation planning and enable coordinated resource mobilisation. We outline development of an investment case for Tanzania to estimate additional financing for scaling up SSNC to 80% of districts as part of health sector strategies to meet the country's targets.
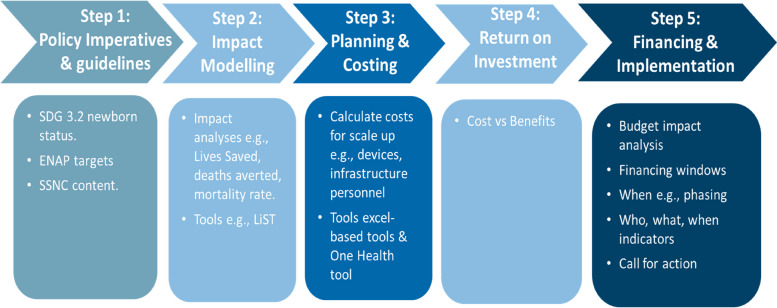
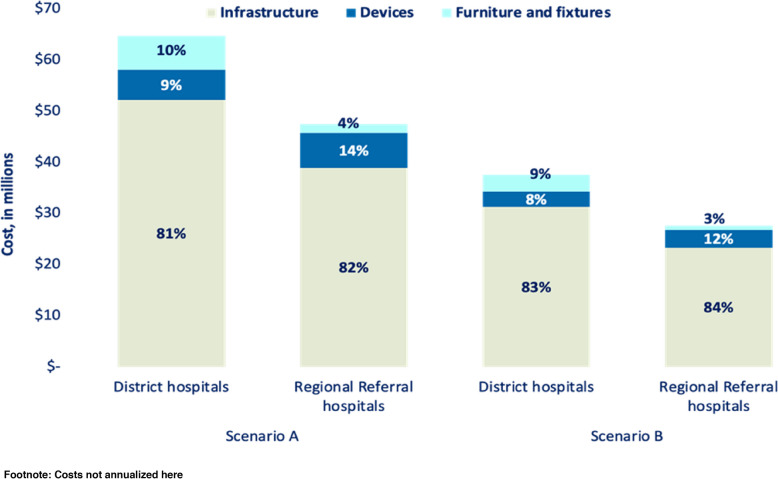
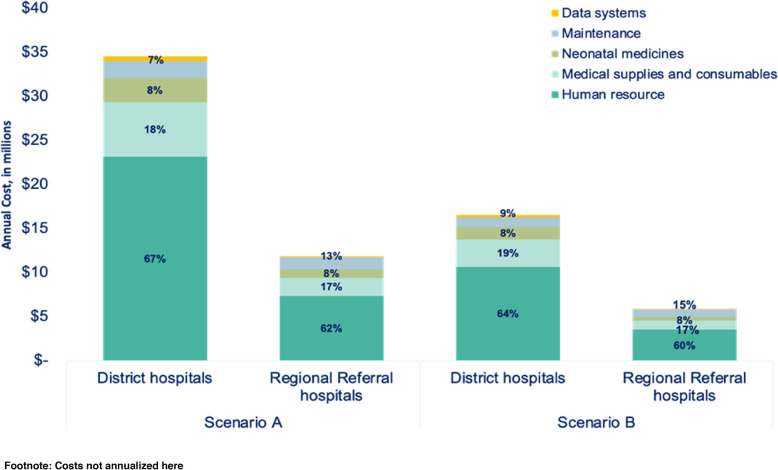
Methods: We followed five steps: (1) reviewed national targets, policies and guidelines; (2) modelled potential health benefits by increased coverage of SSNC using the Lives Saved Tool; (3) estimated setup and running costs using the Neonatal Device Planning and Costing Tool, applying two scenarios: (A) all new neonatal units and devices with optimal staffing, and (B) half new and half modifying, upgrading, or adding resources to existing neonatal units; (4) calculated budget impact and return on investment (ROI) and (5) identified potential financing opportunities.
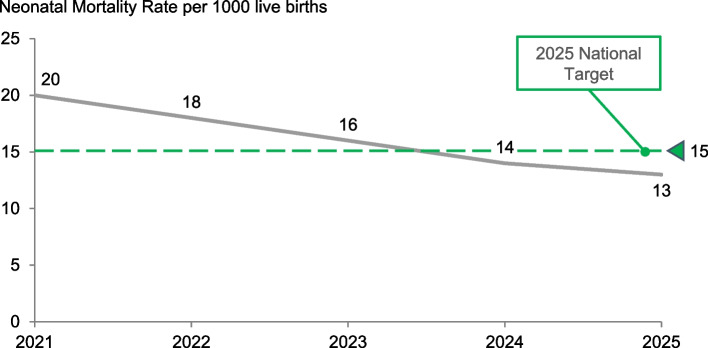
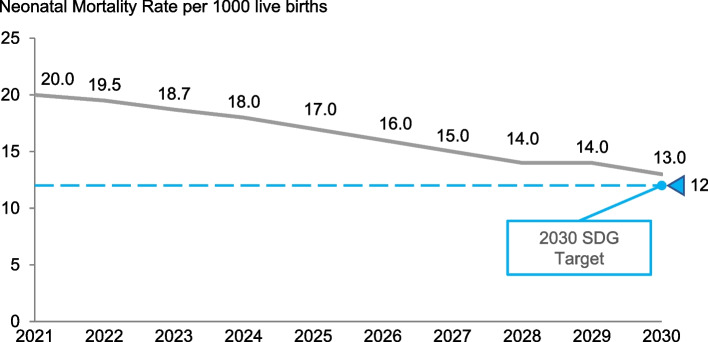
Results: Neonatal mortality rate was forecast to fall from 20 to 13 per 1000 live births with scale-up of SSNC, superseding the government 2025 target of 15, and close to the 2030 Sustainable Development Goal 3.2 target of <12. At 85% endline coverage, estimated cumulative lives saved were 36,600 by 2025 and 80,000 by 2030. Total incremental costs were estimated at US$166 million for scenario A (US$112 million set up and US$54 million for running costs) and US$90 million for scenario B (US$65 million setup and US$25 million for running costs). Setup costs were driven by infrastructure (83%) and running costs by human resources (60%). Cost per capita was US$0.93 and the ROI is estimated to be between US$8-12 for every dollar invested.
Conclusions: ROI for SSNC is higher compared to other health investments, noting many deaths averted followed by full lifespan. This is conservative since disability averted is not included. Budget impact analysis estimated a required 2.3% increase in total government health expenditure per capita from US$40.62 in 2020, which is considered affordable, and the government has already allocated additional funding. Our proposed five-step SSNC investment case has potential for other countries wanting to accelerate progress.
Keywords: Hospital care; Investment case; Low- and middle-income countries; Neonatal; Newborn; Return on investment.
© 2023. The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures

References
-
- UN Interagency Group for Child Mortality Estimation . Levels and trends in child mortality: Report 2022. New York: UN-IGME; 2023.
-
- World Health Organization . Every newborn: an action plan to end preventable deaths. Geneva: WHO; 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
