

Anti-seizure gene therapy for focal cortical dysplasia
- PMID: 38100333
- PMCID: PMC10834237
- DOI: 10.1093/brain/awad387
Anti-seizure gene therapy for focal cortical dysplasia
Abstract
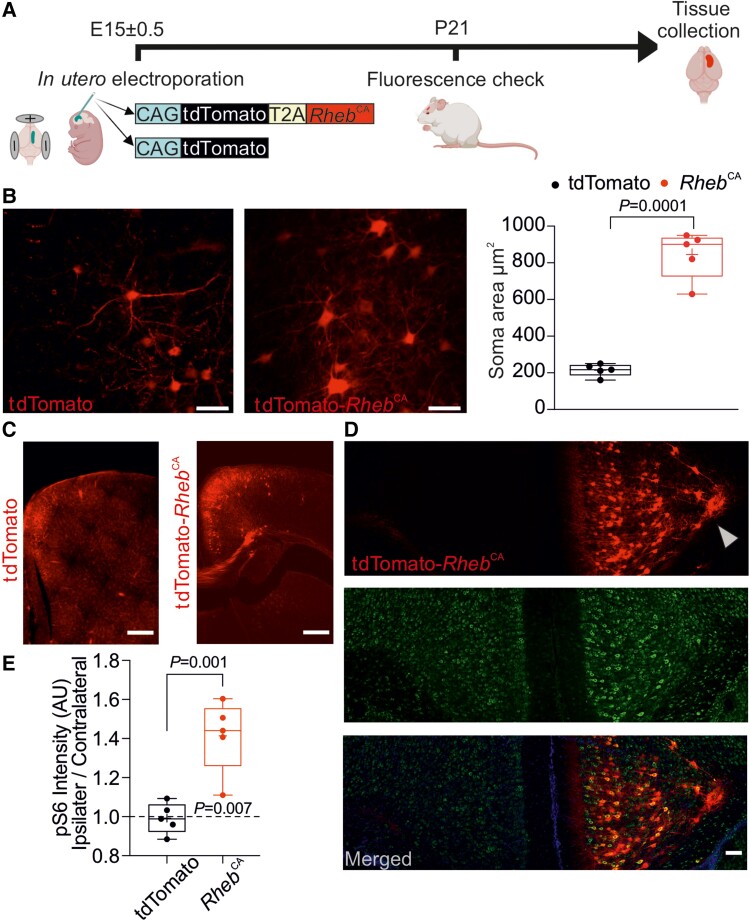
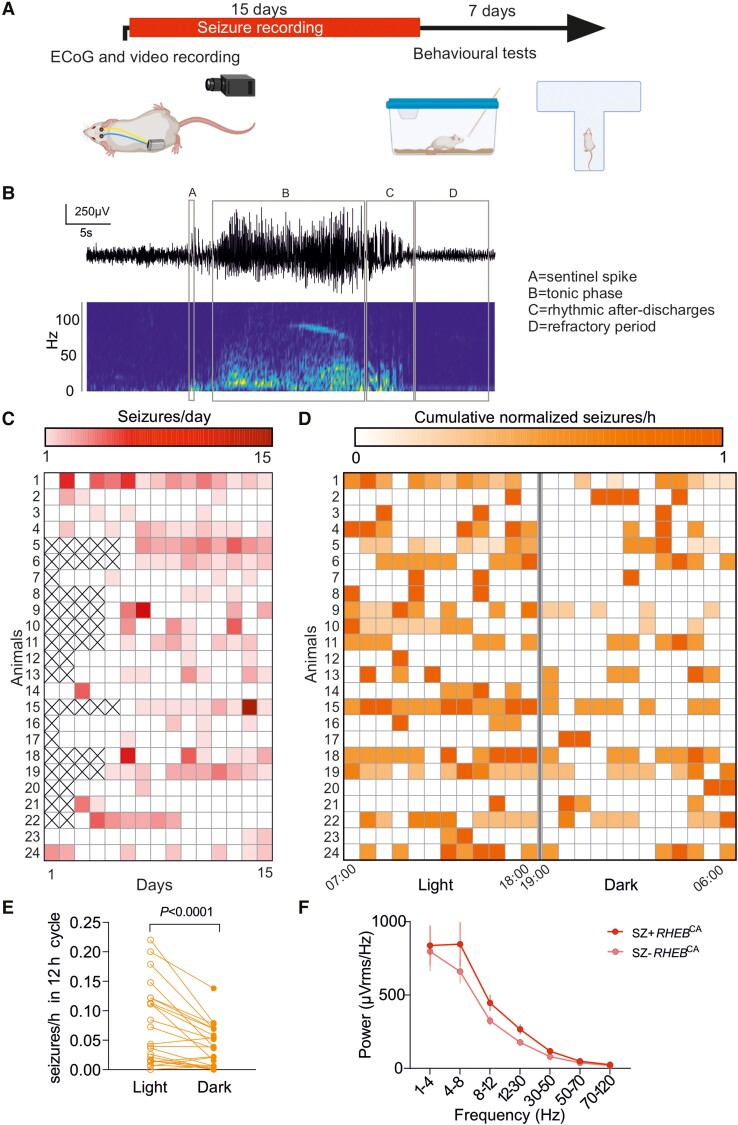
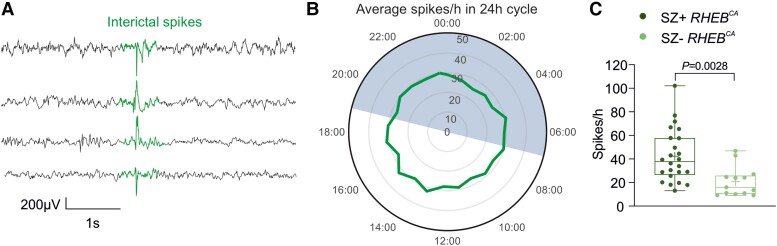
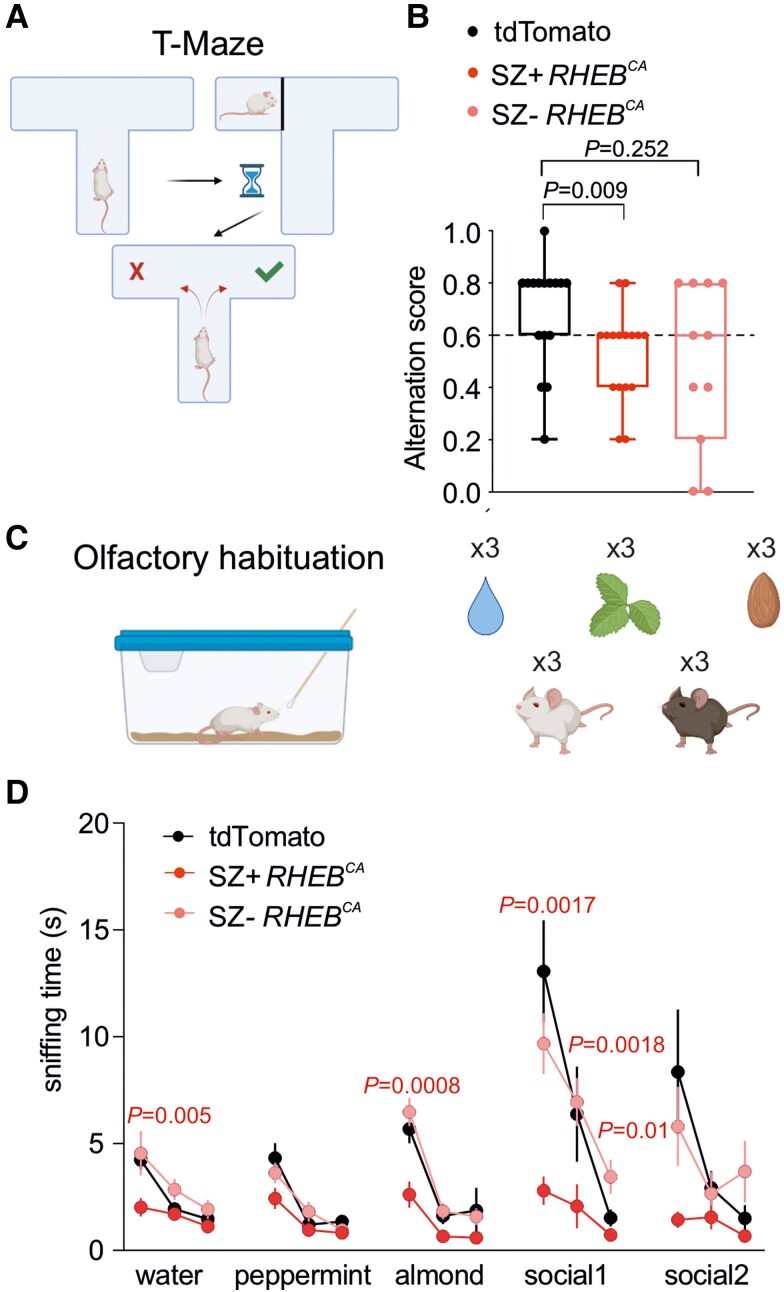
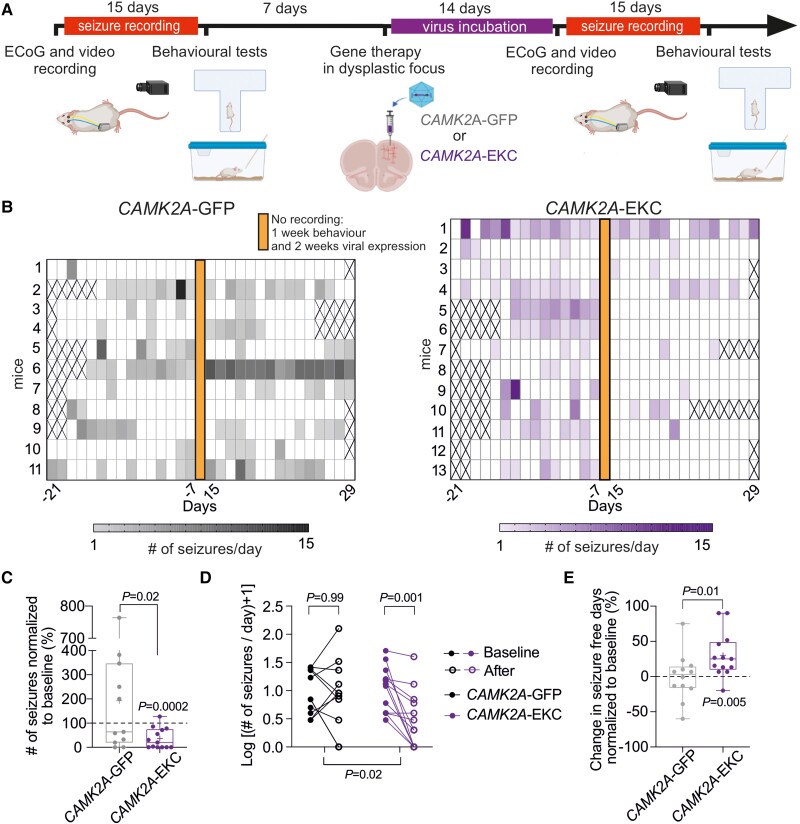
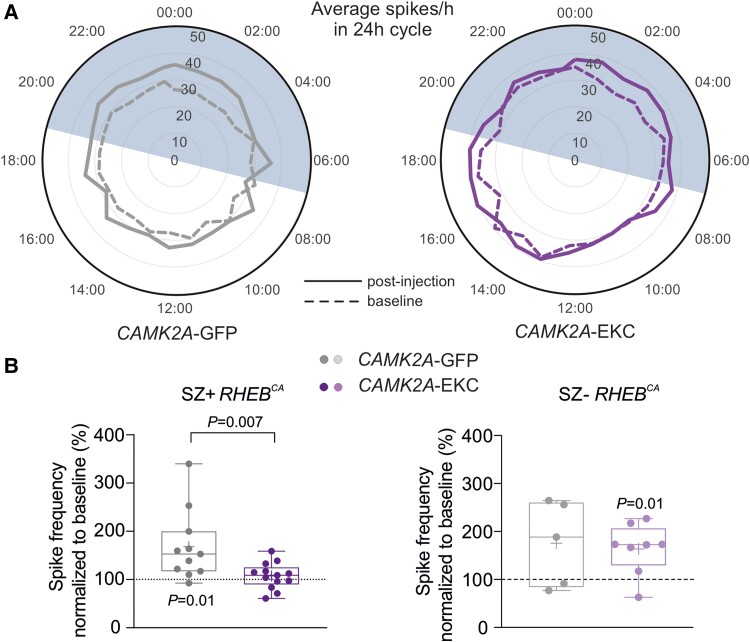
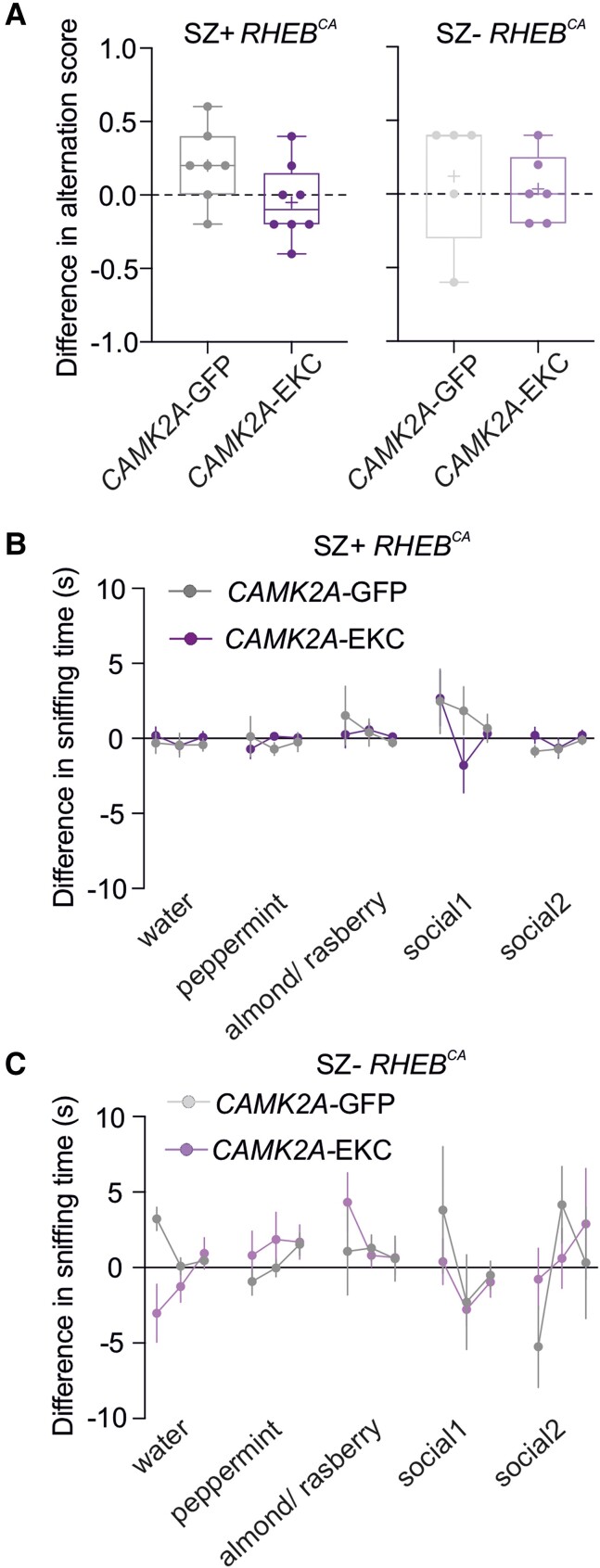
Focal cortical dysplasias are a common subtype of malformation of cortical development, which frequently presents with a spectrum of cognitive and behavioural abnormalities as well as pharmacoresistant epilepsy. Focal cortical dysplasia type II is typically caused by somatic mutations resulting in mammalian target of rapamycin (mTOR) hyperactivity, and is the commonest pathology found in children undergoing epilepsy surgery. However, surgical resection does not always result in seizure freedom, and is often precluded by proximity to eloquent brain regions. Gene therapy is a promising potential alternative treatment and may be appropriate in cases that represent an unacceptable surgical risk. Here, we evaluated a gene therapy based on overexpression of the Kv1.1 potassium channel in a mouse model of frontal lobe focal cortical dysplasia. An engineered potassium channel (EKC) transgene was placed under control of a human promoter that biases expression towards principal neurons (CAMK2A) and packaged in an adeno-associated viral vector (AAV9). We used an established focal cortical dysplasia model generated by in utero electroporation of frontal lobe neural progenitors with a constitutively active human Ras homolog enriched in brain (RHEB) plasmid, an activator of mTOR complex 1. We characterized the model by quantifying electrocorticographic and behavioural abnormalities, both in mice developing spontaneous generalized seizures and in mice only exhibiting interictal discharges. Injection of AAV9-CAMK2A-EKC in the dysplastic region resulted in a robust decrease (∼64%) in the frequency of seizures. Despite the robust anti-epileptic effect of the treatment, there was neither an improvement nor a worsening of performance in behavioural tests sensitive to frontal lobe function. AAV9-CAMK2A-EKC had no effect on interictal discharges or behaviour in mice without generalized seizures. AAV9-CAMK2A-EKC gene therapy is a promising therapy with translational potential to treat the epileptic phenotype of mTOR-related malformations of cortical development. Cognitive and behavioural co-morbidities may, however, resist an intervention aimed at reducing circuit excitability.
Keywords: epilepsy; focal cortical dysplasia; gene therapy; translation.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
D.M.K. and S.S. are listed as inventors on Patent WO2018229254A1. G.L., D.M.K. and S.S. have equity in a company that aims to bring epilepsy gene therapy to the clinic.
Figures
Comment in
-
Gene therapy for seizures in focal cortical dysplasia.Nat Rev Neurol. 2024 Feb;20(2):63. doi: 10.1038/s41582-023-00926-8. Nat Rev Neurol. 2024. PMID: 38167679 No abstract available.
References
-
- Blumcke I, Spreafico R, Haaker G, et al. Histopathological findings in brain tissue obtained during epilepsy surgery. N Engl J Med. 2017;377:1648–1656. - PubMed
-
- Stevelink R, Sanders MWCB, Tuinman M, et al. Epilepsy surgery in patients with genetic refractory epilepsy: A systematic review. Eur J Paediatr Neurol. 2017;21:e17.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
