

Analysis of uterine evacuation methods in postabortion care after implementation of a surveillance network (CLAP MUSA-Network) at a university hospital
- PMID: 38100497
- PMCID: PMC10723722
- DOI: 10.1371/journal.pone.0296009
Analysis of uterine evacuation methods in postabortion care after implementation of a surveillance network (CLAP MUSA-Network) at a university hospital
Abstract
Background: Management of uterine evacuation is essential for increasing safe abortion care. Monitoring through surveillance systems tracks changes in clinical practice and provides information to improve equity in abortion care quality.
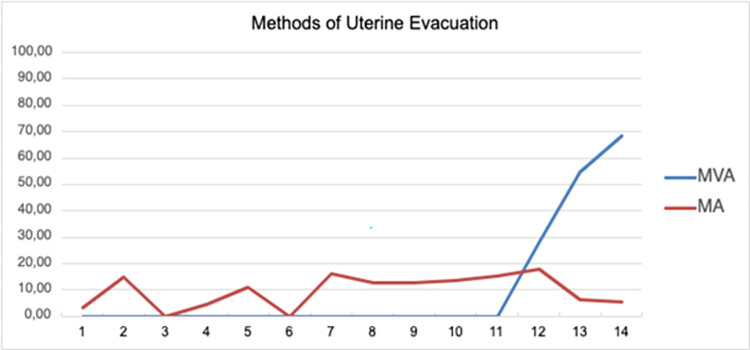
Objective: This study aimed to evaluate the frequency of manual vacuum aspiration (MVA) and medical abortion (MA), and identify the factors associated with each uterine evacuation method after surveillance network installation at a Brazilian hospital.
Methods: This cross-sectional study included women admitted for abortion or miscarriage to the University of Campinas Women's Hospital, Brazil, between July 2017 and November 2020. The dependent variables were the use of MVA and MA with misoprostol. The independent variables were the patients' clinical and sociodemographic data. The Cochran-Armitage, chi-square, and Mann-Whitney U tests, as well as multiple logistic regression analysis, were used to compare uterine evacuation methods.
Results: We enrolled 474 women in the study, 91.35% of whom underwent uterine evacuation via uterine curettage (78.75%), MVA (9.46%), or MA (11.54%). MVA use increased during the study period (Z = 9.85, p < 0.001). Admission in 2020 (odds ratio [OR] 64.22; 95% confidence interval [CI] 3.79-1086.69) and lower gestational age (OR 0.837; 95% CI 0.724-0.967) were independently associated with MVA, whereas the only factor independently associated with MA was a higher education level (OR 2.66; 95% CI 1.30-5.46).
Conclusion: MVA use increased following the installation of a surveillance network for good clinical practice. Being part of a network that encourages the use of evidence-based methods provides an opportunity for healthcare facilities to increase access to safe abortions.
Copyright: © 2023 Veiga-Junior et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Factors Associated with Abortion Complications after the Implementation of a Surveillance Network (MUSA Network) in a University Hospital.Rev Bras Ginecol Obstet. 2021 Jul;43(7):507-512. doi: 10.1055/s-0041-1735129. Epub 2021 Aug 30. Rev Bras Ginecol Obstet. 2021. PMID: 34461660 Free PMC article.
-
Post-abortion contraception before hospital discharge after installation of a surveillance network in Brazil.Int J Gynaecol Obstet. 2020 Aug;150(2):200-205. doi: 10.1002/ijgo.13170. Epub 2020 May 7. Int J Gynaecol Obstet. 2020. PMID: 32304228
-
Replacement of dilation and curettage/evacuation by manual vacuum aspiration and medical abortion, and the introduction of postabortion contraception in Pakistan.Int J Gynaecol Obstet. 2014 Jul;126 Suppl 1:S40-4. doi: 10.1016/j.ijgo.2014.03.016. Epub 2014 Mar 30. Int J Gynaecol Obstet. 2014. PMID: 24743026
-
The cost of post-abortion care (PAC): a systematic review.BMC Health Serv Res. 2022 Mar 25;22(1):391. doi: 10.1186/s12913-022-07765-1. BMC Health Serv Res. 2022. PMID: 35337323 Free PMC article.
-
Methods for induced abortion.Obstet Gynecol. 2004 Jul;104(1):174-85. doi: 10.1097/01.AOG.0000130842.21897.53. Obstet Gynecol. 2004. PMID: 15229018 Review.
References
-
- World Health Organization. Abortion care guideline Geneva: World Health Organization; 2022.
-
- Safe Abortion: Technical and Policy Guidance for Health Systems. 2nd ed. Geneva: World Health Organization; 2012. - PubMed
-
- Diniz D, Medeiros M, Madeiro A. National Abortion Survey—Brazil, 2021. Cien Saude Colet. 2023 Jun;28(6):1601–1606. - PubMed
-
- Cardoso BB, Vieira FMSB, Saraceni V. Abortion in Brazil: what do the official data say?. Cad. Saúde Pública 2020; 36 (1): e00188718. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
