

Immunomodulator use, risk factors and management of flares, and mortality for patients with pre-existing rheumatoid arthritis after immune checkpoint inhibitors for cancer
- PMID: 38100899
- PMCID: PMC10842881
- DOI: 10.1016/j.semarthrit.2023.152335
Immunomodulator use, risk factors and management of flares, and mortality for patients with pre-existing rheumatoid arthritis after immune checkpoint inhibitors for cancer
Abstract
Objective: To investigate immunomodulator use, risk factors and management for rheumatoid arthritis (RA) flares, and mortality for patients with pre-existing RA initiating immune checkpoint inhibitors (ICI) for cancer.
Methods: We performed a retrospective cohort study of all patients with RA meeting 2010 ACR/EULAR criteria that initiated ICI for cancer at Mass General Brigham or Dana-Farber Cancer Institute in Boston, MA (2011-2022). We described immunomodulator use and changes at baseline of ICI initiation. We identified RA flares after baseline, categorized the severity, and described the management. Baseline factors were examined for RA flare risk using Fine and Gray competing risk models. We performed a landmark analysis to limit the potential for immortal time bias, where the analysis started 3 months after ICI initiation. Among those who survived at least 3 months, we examined whether RA flare within 3 months after ICI initiation was associated with mortality using Cox regression.
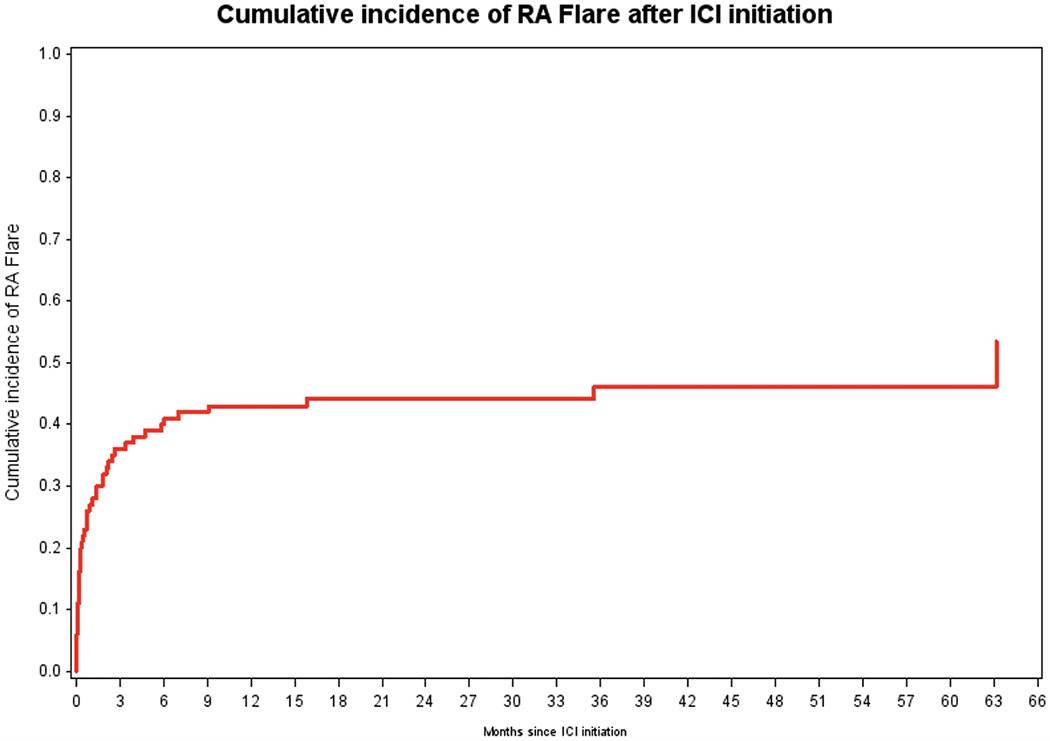
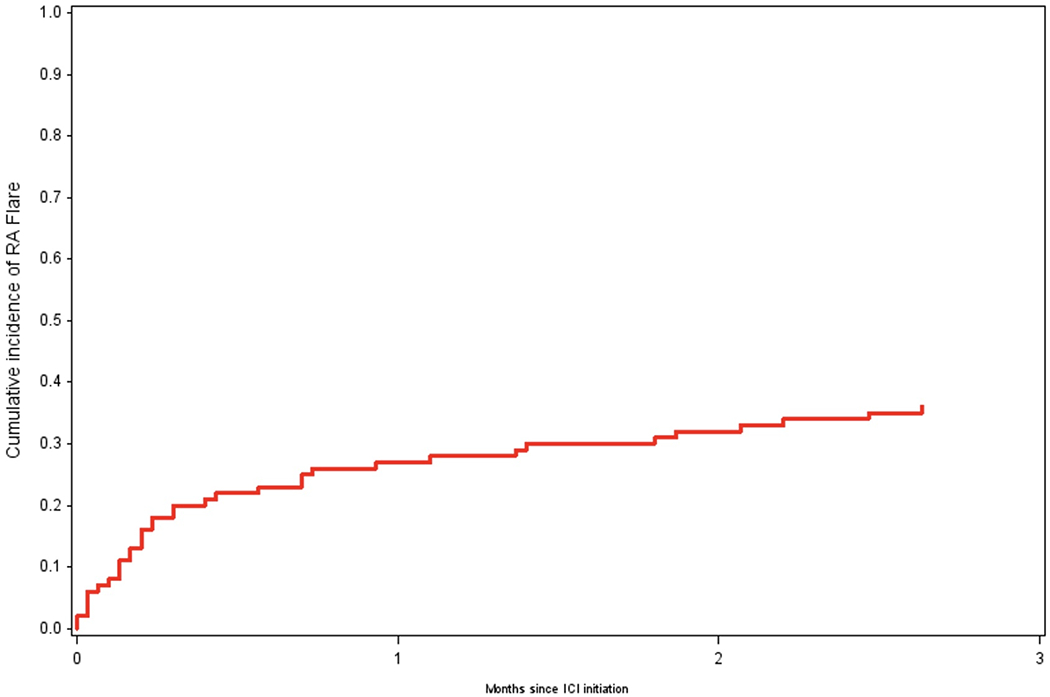
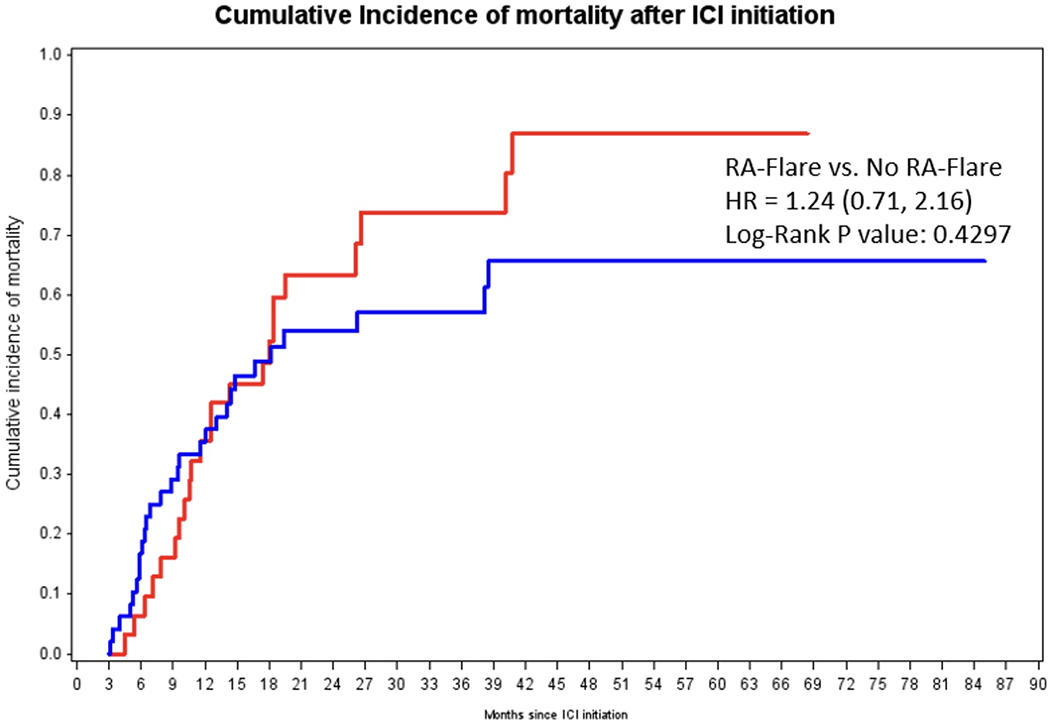
Results: Among 11,901 patients who initiated ICI for cancer treatment, we analyzed 100 pre-existing RA patients (mean age 70.3 years, 63 % female, 89 % on PD-1 monotherapy, 50 % lung cancer). At ICI initiation, 71 % were seropositive, 82 % had remission/low RA disease activity, 24 % were on glucocorticoids, 35 % were on conventional synthetic disease-modifying antirheumatic drugs (DMARDs), and 10 % were on biologic or targeted synthetic DMARDs. None discontinued glucocorticoids and 3/35 (9 %) discontinued DMARDs in anticipation of starting ICI. RA flares occurred in 46 % (incidence rate 1.84 per 1000 person-months, 95 % CI 1.30, 2.37); 31/100 flared within 3 months of baseline. RA flares were grade 1 in 16/46 (35 %), grade 2 in 25/46 (54 %), and grade 3 in 5/46 (11 %); 2/46 (4 %) required hospitalization for RA flare. Concomitant immune-related adverse events occurred in 15/46 (33 %) that flared. A total of 72/100 died during follow-up; 21 died within 3 months of baseline. Seropositivity had an age-adjusted sdHR of 1.95 (95 % CI 1.02, 3.71) for RA flare compared to seronegativity, accounting for competing risk of death. Otherwise, no baseline factors were associated with RA flare, including cancer type, disease activity, RA duration, and deformities. 9/46 (20 %) patients had their ICI discontinued/paused due to RA flares. In the landmark analysis among 79 patients who survived at least 3 months, RA flare in the first 3 months was not associated with lower mortality (adjusted HR 1.24, 95 % CI 0.71, 2.16) compared to no RA flare.
Conclusion: Among patients with pre-existing RA, few changed immunomodulator medications in anticipation of starting ICI, but RA flares occurred in nearly half. RA flares were mostly mild and treated with typical therapies. Seropositivity was associated with RA flare risk. A minority had severe RA flares requiring disruption of ICI, and RA flares were not associated with mortality.
Keywords: Cancer; Flare; Immune checkpoint inhibitors; Immunotherapy; Rheumatoid arthritis.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest Dr. Yoshida has performed consultancy for OM1, Inc. Dr. LeBoeuf has performed consultancy for Bayer, Seattle Genetics, Sanofi, Silverback, and Synox Therapeutics. Dr. Buchbinder serves on an advisory board for Merck, BMS, and Novartis. Dr. Gedmintas has received payment for lectures for Harvard CME of Intensive Review of Internal Medicine and Innovations and New Practices in Internal Medicine. Dr. Rao has received research support from Bristol Myers Squibb, Janssen, and Merck, and performed consultancy for AstraZeneca, Pfizer, GlaxoSmithKine, Aditum, HiFiBio Therapeutics, and Scipher Medicine unrelated to this work. Dr. Gravallese has received grants from the NIH and Rheumatology Research Foundation. Dr. Gravallese has received royalties from Up to Date and textbook “Rheumatology.” Dr. Gravallese has received payment for speaking at IFRA meeting China, Advances in Targeted Therapies Meeting, University of NC, MUSC, and ACR. Dr. Gravallese has received support for attending meeting with Advances in Targeted Therapies and the NIH. Dr. Gravallese serves in a leadership role for the NIH and NIAMs Council member. Dr. Sparks has received research support from Bristol Myers Squibb and performed consultancy for AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Gilead, Inova Diagnostics, Janssen, Optum, Pfizer, and ReCor unrelated to this work. The funders had no role in the decision to publish or preparation of this manuscript. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard University, its affiliated academic health care centers, or the National Institutes of Health.
Figures
Similar articles
-
Mortality and immune-related adverse events after immune checkpoint inhibitor initiation for cancer among patients with pre-existing rheumatoid arthritis: a retrospective, comparative, cohort study.Lancet Rheumatol. 2023 May;5(5):e274-e283. doi: 10.1016/s2665-9913(23)00064-4. Epub 2023 Mar 27. Lancet Rheumatol. 2023. PMID: 37841635 Free PMC article.
-
Immune Checkpoint Inhibitor Associated Rheumatoid Arthritis.Curr Rheumatol Rep. 2024 Nov 26;27(1):3. doi: 10.1007/s11926-024-01173-6. Curr Rheumatol Rep. 2024. PMID: 39589663 Review.
-
Risk of Toxicity After Initiating Immune Checkpoint Inhibitor Treatment in Patients With Rheumatoid Arthritis.J Clin Rheumatol. 2021 Oct 1;27(7):267-271. doi: 10.1097/RHU.0000000000001314. J Clin Rheumatol. 2021. PMID: 31977647 Free PMC article.
-
Predictors of Rheumatic Immune-Related Adverse Events and De Novo Inflammatory Arthritis After Immune Checkpoint Inhibitor Treatment for Cancer.Arthritis Rheumatol. 2022 Mar;74(3):527-540. doi: 10.1002/art.41949. Epub 2022 Jan 25. Arthritis Rheumatol. 2022. PMID: 34397169 Free PMC article.
-
Treatment of immune checkpoint inhibitor-induced inflammatory arthritis.Curr Opin Rheumatol. 2020 May;32(3):315-320. doi: 10.1097/BOR.0000000000000701. Curr Opin Rheumatol. 2020. PMID: 32168068 Free PMC article. Review.
Cited by
-
Immune checkpoint inhibitors and rheumatoid arthritis: All roads lead to PD-1?Semin Arthritis Rheum. 2025 Feb;70S:152582. doi: 10.1016/j.semarthrit.2024.152582. Epub 2024 Nov 14. Semin Arthritis Rheum. 2025. PMID: 39578183 Review.
-
Use of Upadacitinib to Treat a Severe Flare-Up of Rheumatoid Arthritis During Anti-PD-1 Immune Checkpoint Inhibitor Therapy for Stage IV Squamous Cell Carcinoma of the Lung.J Clin Med. 2024 Oct 20;13(20):6257. doi: 10.3390/jcm13206257. J Clin Med. 2024. PMID: 39458207 Free PMC article.
-
Immune checkpoint inhibitors in cancer patients with autoimmune disease: Safety and efficacy.Hum Vaccin Immunother. 2025 Dec;21(1):2458948. doi: 10.1080/21645515.2025.2458948. Epub 2025 Feb 2. Hum Vaccin Immunother. 2025. PMID: 39894761 Free PMC article.
References
-
- Ghosh N, Bass AR. Rheumatic Complications of Immune Checkpoint Inhibitors. Rheum Dis Clin North Am 2022; 48(2): 411–28. - PubMed
-
- van der Kooij MK, Suijkerbuijk KPM, Aarts MJB, et al. Safety and Efficacy of Checkpoint Inhibition in Patients With Melanoma and Preexisting Autoimmune Disease : A Cohort Study. Ann Intern Med 2021; 174(5): 641–8. - PubMed
-
- Abdel-Wahab N, Shah M, Lopez-Olivo MA, Suarez-Almazor ME. Use of Immune Checkpoint Inhibitors in the Treatment of Patients With Cancer and Preexisting Autoimmune Disease: A Systematic Review. Ann Intern Med 2018; 168(2): 121–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
