

Concomitant Treatment of Atrial Fibrillation in Isolated Coronary Artery Bypass Grafting
- PMID: 38101594
- PMCID: PMC11055678
- DOI: 10.1016/j.athoracsur.2023.11.034
Concomitant Treatment of Atrial Fibrillation in Isolated Coronary Artery Bypass Grafting
Abstract
Background: Societal guidelines support concomitant management of atrial fibrillation (AF) in patients undergoing cardiac surgery. To assess real-world adoption and outcomes, this study evaluated Medicare beneficiaries with AF who underwent isolated coronary artery bypass grafting (CABG) with surgical ablation (SA) or left atrial appendage obliteration (LAAO) or both procedures in combination (SA + LAAO).
Methods: The US Centers for Medicare & Medicaid Services inpatient claims database identified all patients with AF who underwent isolated CABG from 2018 to 2020. Diagnosis-related group and International Classification of Diseases-10th revision procedure codes defined covariates for doubly robust risk adjustment.
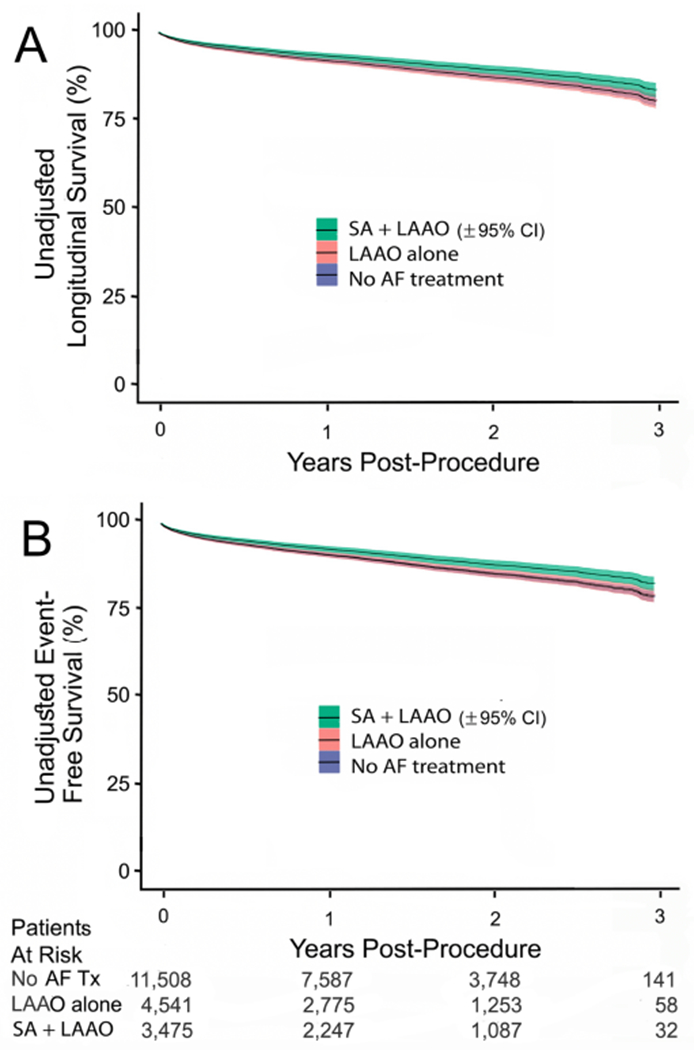
Results: A total of 19,524 patients with preoperative AF who underwent isolated CABG were stratified by SA + LAAO (3475 patients; 17.8%), LAAO only (4541 patients; 23.3%), or no AF treatment (11,508 patients; 58.9%). After doubly robust risk adjustment, longitudinal analysis highlighted that concomitant AF treatment with SA + LAAO (hazard ratio [HR], 0.74; P = .049) or LAAO alone (HR, 0.75; P = . 031) was associated with a significant reduction in readmission for stroke at 3 years compared with no AF treatment. Furthermore, SA + LAAO (HR, 0.86; P = .016) but not LAAO alone (HR, 0.97; P = .573) was associated with improved survival compared with no AF treatment. Finally, SA + LAAO was associated with a superior composite outcome of freedom from stroke or death at 3 years compared with LAAO alone (HR, 0.86;, P = .033) or no AF treatment (HR, 0.81; P = .001).
Conclusions: In Medicare beneficiaries with AF who underwent isolated CABG, concomitant AF treatment was associated with reduced 3-year readmission for stroke. SA + LAAO was associated with superior reduction in stroke or death at 3 years compared with LAAO alone or no AF treatment.
Copyright © 2024 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests:
Figures



References
-
- Badhwar V, Rankin JS, Damiano RJ Jr. et al. The society of thoracic surgeons 2017 clinical practice guidelines for the surgical treatment of atrial fibrillation. Ann Thorac Surg 2017;103(1):329–341. - PubMed
-
- Badhwar V, Rankin JS, Ad N et al. Surgical ablation of atrial fibrillation in the united states: Trends and propensity matched outcomes. Ann Thorac Surg 2017;104(2):493–500. - PubMed
-
- Mao Z, Zhong X, Yin J, Zhao Z, Hu X, Hackett ML. Predictors associated with stroke after coronary artery bypass grafting: A systematic review. J Neurol Sci 2015;357(1-2):1–7. - PubMed
-
- Rankin JS, Lerner DJ, Braid-Forbes MJ, Ferguson MA, Badhwar V. One-year mortality and costs associated with surgical ablation for atrial fibrillation concomitant to coronary artery bypass grafting. Eur J Cardiothorac Surg 2017;52(3):471–477. - PubMed
-
- Badhwar V, Scott Rankin J, Lee R, McCarthy PM, Wei LM. Contemporary left atrial appendage management during adult cardiac surgery. J Thorac Cardiovasc Surg 2022. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
