

Comparing outcomes between coronary artery bypass grafting and percutaneous coronary intervention in octogenarians with left main or multivessel disease
- PMID: 38102297
- PMCID: PMC10724226
- DOI: 10.1038/s41598-023-49069-2
Comparing outcomes between coronary artery bypass grafting and percutaneous coronary intervention in octogenarians with left main or multivessel disease
Abstract
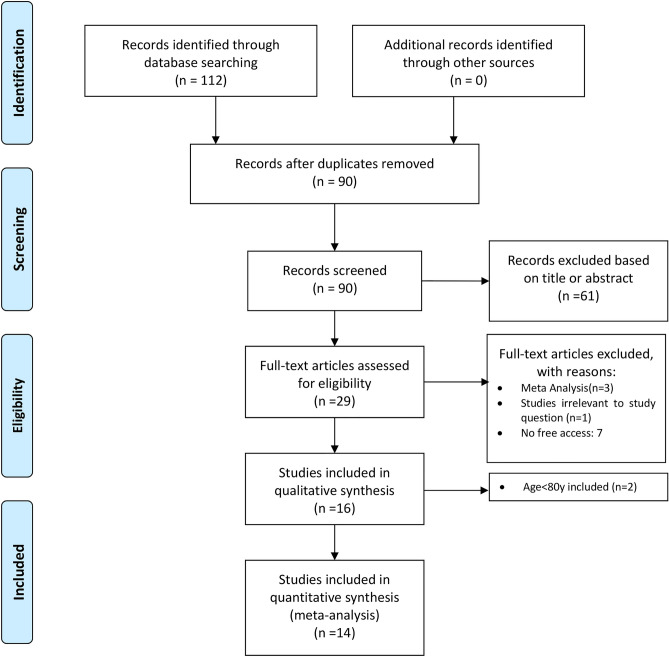
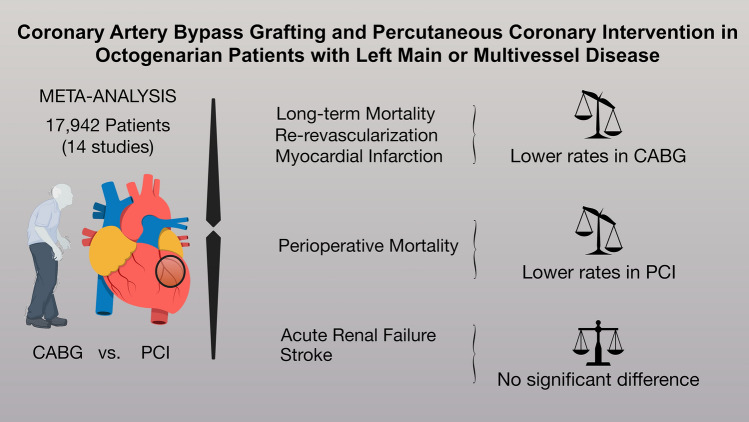
Mechanisms of coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) differ as CABG provides surgical collateralization and may prolong life by preventing future myocardial infarctions (MI). However, CABG benefits are unclear in octogenarians, where surgical risk is often perceived as higher and PCI is chosen more liberally. We performed a meta-analysis of studies comparing outcomes in octogenarians with left main or multivessel disease who underwent CABG or PCI. Primary outcome was late mortality (> 5 years). Secondary outcomes were perioperative mortality, MI, re-revascularization (R-R), acute renal failure (ARF), and stroke. Fourteen studies with 17,942 patients were included. CABG was associated with lower late mortality (hazard ratio, HR: 1.23, 95% confidence interval: CI 1.05-1.44, p < 0.01). In the pooled Kaplan-Meier analysis CABG showed significantly lower risk of death in the follow-up compared to PCI (HR: 1.08, 95%CI 1.02-1.41, p = 0.005). Landmark analyses confirmed the survival advantage of CABG over PCI after 21.5 months of follow-up (HR: 1.31, 1.19-1.44, p < 0.0001), but suggested advantage of PCI over CABG in the first 30-days (HR: 0.72, 0.64-0.82, p < 0.0001) and comparable survival from 1 to 21.5 months (HR: 0.98, 0.92-1.05, p = 0.652). We found lower risk for MI and R-R after CABG but higher perioperative mortality and no differences in ARF and stroke. CABG appears superior to PCI over time in octogenarians with complex CAD. This survival advantage is associated with fewer events of MI and R-R; however, it comes with an increased risk in perioperative mortality.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Gaudino M, Di Franco A, Spadaccio C, et al. Difference in spontaneous myocardial infarction and mortality in percutaneous versus surgical revascularization trials: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2021;165:662–669.e14. doi: 10.1016/j.jtcvs.2021.04.062. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
