

Postoperative thrombotic events following major surgery in patients with a history of COVID-19: a retrospective cohort analysis of commercially insured beneficiaries in the USA
- PMID: 38102451
- PMCID: PMC10858061
- DOI: 10.1007/s12630-023-02639-4
Postoperative thrombotic events following major surgery in patients with a history of COVID-19: a retrospective cohort analysis of commercially insured beneficiaries in the USA
Abstract
Purpose: We sought to evaluate the synergistic risk of postoperative thrombosis in patients with a history of COVID-19 who undergo major surgery. Major surgery and SARS-CoV-2 infection are independently associated with an increased risk of thrombosis, but the magnitude of additional risk beyond surgery conferred by a COVID-19 history on the development of perioperative thrombotic events has not been clearly elucidated in the literature.
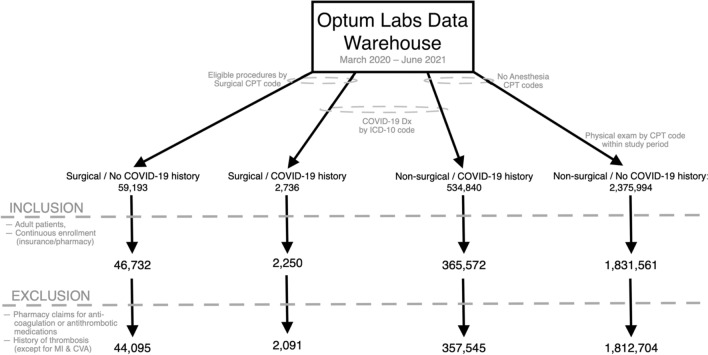
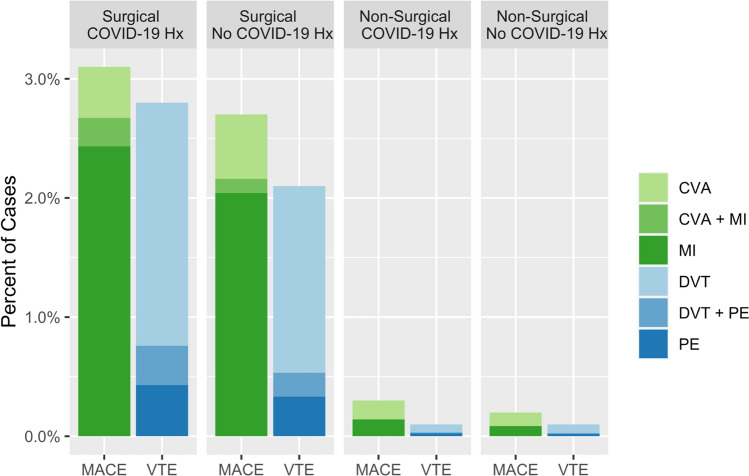
Methods: We conducted a retrospective cohort study among commercially insured adults in the USA from March 2020 to June 2021 using the Optum Labs Data Warehouse (OLDW), a longitudinal, real-world data asset containing deidentified administrative claims and electronic health records. We compared patients with prior COVID-19 who underwent surgery with control individuals who underwent surgery without a COVID-19 history and with control individuals who did not undergo surgery with and without a COVID-19 history. We assessed the interaction of surgery and previous COVID-19 on perioperative thrombotic events (venous thromboembolism and major adverse cardiovascular events) within 90 days using multivariable logistic regression and interaction analysis.
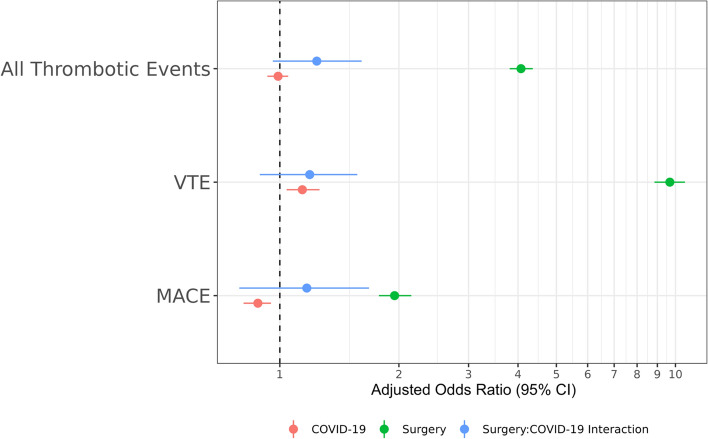
Results: Two million and two-hundred thousand eligible patients were identified from the OLDW. Patients in the surgical cohorts were older and more medically complex than nonsurgical population controls. After adjusting for confounders, only surgical exposure-not COVID-19 history-remained associated with perioperative thrombotic events (adjusted odds ratio [aOR], 4.07; 95% confidence interval [CI], 3.81 to 4.36). The multiplicative interaction term (aOR, 1.25; 95% CI, 0.96 to 1.61) and the synergy index (0.76; 95% CI, 0.56 to 1.04) suggest minimal effect modification of prior COVID-19 on surgery with regards to overall thrombotic risk.
Conclusions: We found no evidence of synergistic thrombotic risk from previous COVID-19 in patients who underwent selected major surgery relative to the baseline thrombotic risk from surgery alone.
RéSUMé: OBJECTIF: Nous avons cherché à évaluer le risque synergique de thrombose postopératoire chez les patient·es ayant des antécédents de COVID-19 qui bénéficient d’une intervention chirurgicale majeure. La chirurgie majeure et l’infection par le SRAS-CoV-2 sont indépendamment associées à un risque accru de thrombose, mais l’ampleur du risque supplémentaire d’apparition de complications thrombotiques périopératoires, au-delà de la chirurgie et conféré par des antécédents de COVID-19, n’a pas été clairement élucidée dans la littérature. MéTHODE: Nous avons mené une étude de cohorte rétrospective auprès d’adultes assuré·es commercialement aux États-Unis de mars 2020 à juin 2021 à l’aide de la base de données Optum Labs Data Warehouse (OLDW), un actif de données longitudinales du monde réel contenant des requêtes administratives anonymisées et des dossiers de santé électroniques. Nous avons comparé les patient·es ayant déjà souffert de COVID-19 et ayant bénéficié d’une intervention chirurgicale avec des personnes témoins ayant bénéficié d’une intervention chirurgicale sans antécédents de COVID-19 et avec des personnes témoins n’ayant pas bénéficié de chirurgie, avec et sans antécédents de COVID-19. Nous avons évalué l’interaction de la chirurgie et des antécédents de COVID-19 avec les complications thrombotiques périopératoires (thromboembolie veineuse et événements cardiovasculaires indésirables majeurs) dans les 90 jours à l’aide d’une régression logistique multivariée et d’une analyse des interactions. RéSULTATS: Deux millions deux cent mille personnes admissibles ont été identifiées à partir du registre OLDW. Les patient·es des cohortes chirurgicales étaient plus âgé·es et présentaient une plus grande complexité médicale que les personnes témoins de la population non chirurgicale. Après ajustement pour tenir compte des facteurs de confusion, seule l’exposition chirurgicale – et non les antécédents de COVID-19 – est restée associée aux complications thrombotiques périopératoires (rapport de cotes ajusté [RCa], 4,07; intervalle de confiance [IC] à 95 %, 3,81 à 4,36). Le terme d’interaction multiplicative (RCa, 1,25; IC 95 %, 0,96 à 1,61) et l’indice de synergie (0,76; IC 95 %, 0,56 à 1,04) suggèrent une modification minimale de l’effet d’un diagnostic antérieur de COVID-19 sur la chirurgie en matière de risque thrombotique global. CONCLUSION: Nous n’avons trouvé aucune preuve de risque thrombotique synergique lié à une COVID-19 antérieure chez les patient·es ayant bénéficié d’une intervention chirurgicale par rapport au risque thrombotique de base lié à la chirurgie seule.
Keywords: COVID-19; SARS-CoV-2; perioperative complications; thrombosis.
© 2023. The Author(s).
Conflict of interest statement
None.
Figures
Similar articles
-
Incidence of venous thrombotic events and events of special interest in a retrospective cohort of commercially insured US patients.BMJ Open. 2022 Feb 9;12(2):e054669. doi: 10.1136/bmjopen-2021-054669. BMJ Open. 2022. PMID: 35140157 Free PMC article.
-
Risks of major arterial and venous thrombotic diseases after hospitalisation for influenza, pneumonia, and COVID-19: A population-wide cohort in 2.6 million people in Wales.Thromb Res. 2025 Jan;245:109213. doi: 10.1016/j.thromres.2024.109213. Epub 2024 Nov 19. Thromb Res. 2025. PMID: 39608301
-
COVID-19 (SARS-CoV-2) infection and thrombotic conditions: A systematic review and meta-analysis.Eur J Clin Invest. 2021 Jun;51(6):e13559. doi: 10.1111/eci.13559. Epub 2021 Apr 14. Eur J Clin Invest. 2021. PMID: 33772772 Free PMC article.
-
Early postoperative COVID infection is associated with significantly increased risk of venous thromboembolism after metabolic and bariatric surgery.Surg Obes Relat Dis. 2024 Aug;20(8):730-736. doi: 10.1016/j.soard.2024.01.021. Epub 2024 Feb 8. Surg Obes Relat Dis. 2024. PMID: 38556419
-
Risk of thromboembolism in patients with COVID-19 who are using hormonal contraception.Cochrane Database Syst Rev. 2023 May 15;5(5):CD014908. doi: 10.1002/14651858.CD014908.pub3. Cochrane Database Syst Rev. 2023. PMID: 37184292 Free PMC article. Review.
Cited by
-
Comparison of early perioperative outcomes of robotic assisted bariatric surgery vs laparoscopic bariatric surgery in a center of excellence.Surg Endosc. 2025 Jul;39(7):4608-4614. doi: 10.1007/s00464-025-11852-9. Epub 2025 Jun 20. Surg Endosc. 2025. PMID: 40542137
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
