

Autoinflammatory Keratinization Diseases-The Concept, Pathophysiology, and Clinical Implications
- PMID: 38103162
- PMCID: PMC10847199
- DOI: 10.1007/s12016-023-08971-3
Autoinflammatory Keratinization Diseases-The Concept, Pathophysiology, and Clinical Implications
Abstract
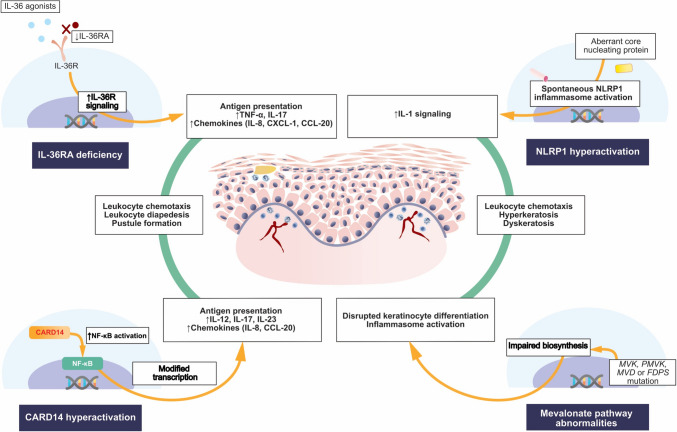
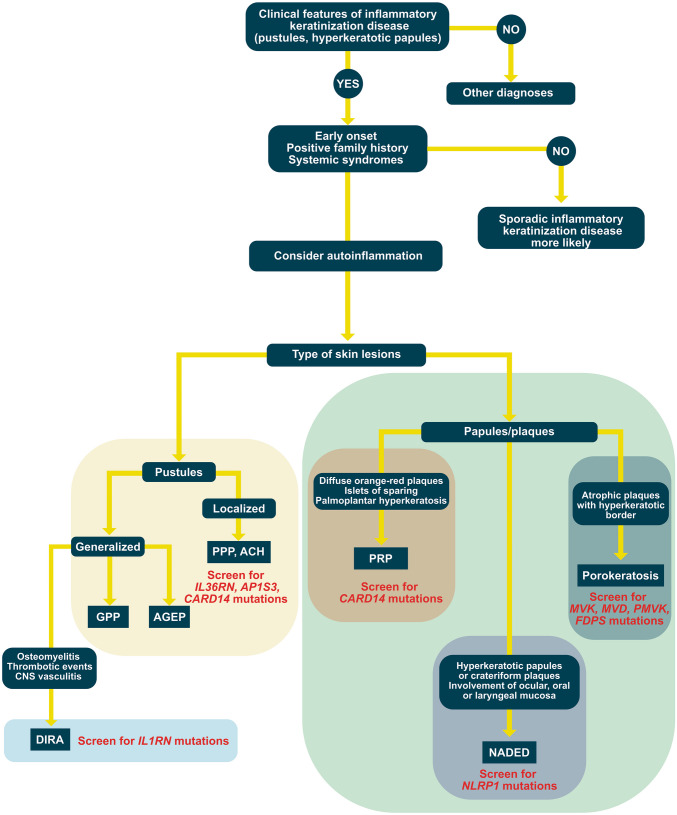
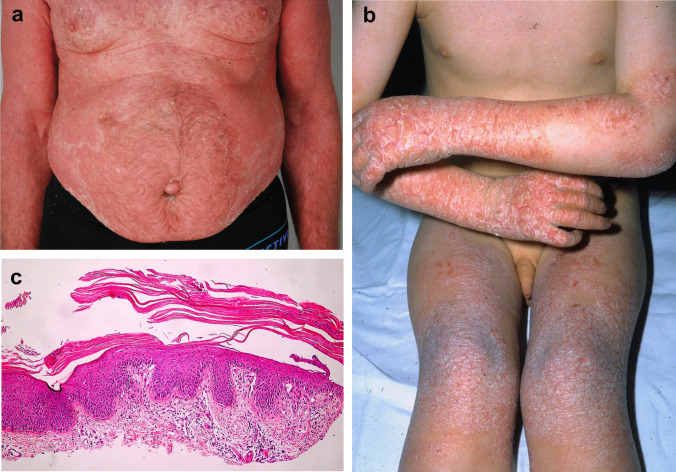
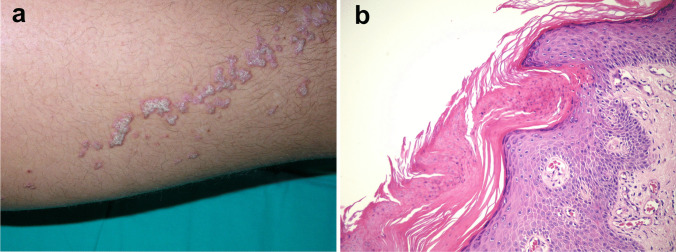
Recent advances in medical genetics elucidated the background of diseases characterized by superficial dermal and epidermal inflammation with resultant aberrant keratosis. This led to introducing the term autoinflammatory keratinization diseases encompassing entities in which monogenic mutations cause spontaneous activation of the innate immunity and subsequent disruption of the keratinization process. Originally, autoinflammatory keratinization diseases were attributed to pathogenic variants of CARD14 (generalized pustular psoriasis with concomitant psoriasis vulgaris, palmoplantar pustulosis, type V pityriasis rubra pilaris), IL36RN (generalized pustular psoriasis without concomitant psoriasis vulgaris, impetigo herpetiformis, acrodermatitis continua of Hallopeau), NLRP1 (familial forms of keratosis lichenoides chronica), and genes of the mevalonate pathway, i.e., MVK, PMVK, MVD, and FDPS (porokeratosis). Since then, endotypes underlying novel entities matching the concept of autoinflammatory keratinization diseases have been discovered (mutations of JAK1, POMP, and EGFR). This review describes the concept and pathophysiology of autoinflammatory keratinization diseases and outlines the characteristic clinical features of the associated entities. Furthermore, a novel term for NLRP1-associated autoinflammatory disease with epithelial dyskeratosis (NADED) describing the spectrum of autoinflammatory keratinization diseases secondary to NLRP1 mutations is proposed.
Keywords: Autoinflammation; Autoinflammatory keratinization diseases; CARD14; IL36RN; NADED; NLRP1.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Autoinflammatory keratinization diseases: An emerging concept encompassing various inflammatory keratinization disorders of the skin.J Dermatol Sci. 2018 May;90(2):105-111. doi: 10.1016/j.jdermsci.2018.01.012. Epub 2018 Feb 1. J Dermatol Sci. 2018. PMID: 29422292 Review.
-
Autoinflammatory keratinitzation diseases (AIKDs.Actas Dermosifiliogr (Engl Ed). 2021 Jun 9:S0001-7310(21)00208-8. doi: 10.1016/j.ad.2021.05.015. Online ahead of print. Actas Dermosifiliogr (Engl Ed). 2021. PMID: 34118208 Review. English, Spanish.
-
The genetic background of generalized pustular psoriasis: IL36RN mutations and CARD14 gain-of-function variants.J Dermatol Sci. 2014 Jun;74(3):187-92. doi: 10.1016/j.jdermsci.2014.02.006. Epub 2014 Mar 5. J Dermatol Sci. 2014. PMID: 24656634 Review.
-
Pustular psoriasis and related pustular skin diseases.Br J Dermatol. 2018 Mar;178(3):614-618. doi: 10.1111/bjd.16232. Epub 2018 Jan 15. Br J Dermatol. 2018. PMID: 29333670 Review.
-
[Autoinflammatory diseases in dermatology: DITRA and CAMPS].Nihon Rinsho Meneki Gakkai Kaishi. 2017;40(3):169-173. doi: 10.2177/jsci.40.169. Nihon Rinsho Meneki Gakkai Kaishi. 2017. PMID: 28747603 Review. Japanese.
Cited by
-
RNF20/RNF40 supports the aggressive behavior in cervical cancer by regulating a peroxisome-based anti-ferroptotic mechanism.Cell Commun Signal. 2025 Jul 1;23(1):304. doi: 10.1186/s12964-025-02279-9. Cell Commun Signal. 2025. PMID: 40597205 Free PMC article.
-
Efficacy and safety of small molecule drugs in the treatment of pityriasis rubra pilaris-A systematic review.Front Med (Lausanne). 2025 Feb 25;12:1544197. doi: 10.3389/fmed.2025.1544197. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40093023 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
