

An umbrella review of effectiveness and efficacy trials for app-based health interventions
- PMID: 38104213
- PMCID: PMC10725431
- DOI: 10.1038/s41746-023-00981-x
An umbrella review of effectiveness and efficacy trials for app-based health interventions
Abstract
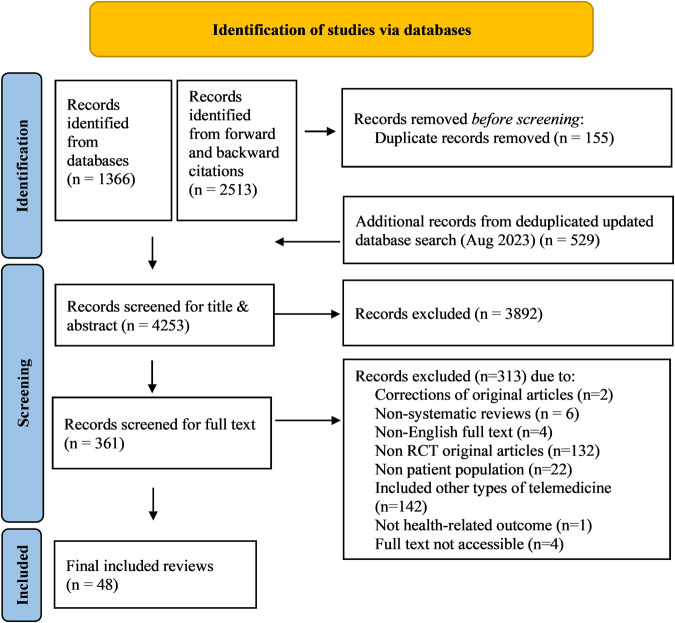
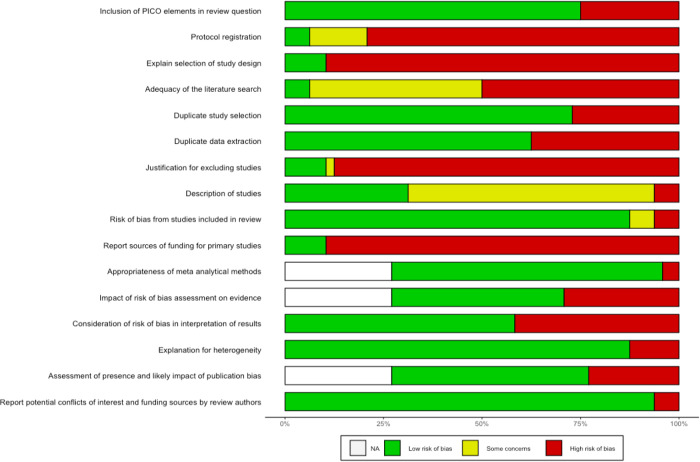
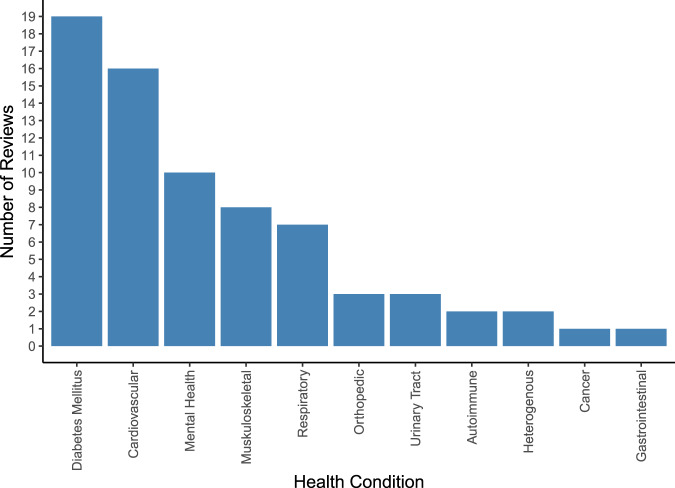
Health interventions based on mobile phone or tablet applications (apps) are promising tools to help patients manage their conditions more effectively. Evidence from randomized controlled trials (RCTs) on efficacy and effectiveness of such interventions is increasingly available. This umbrella review aimed at mapping and narratively summarizing published systematic reviews on efficacy and effectiveness of mobile app-based health interventions within patient populations. We followed a pre-specified publicly available protocol. Systematic reviews were searched in two databases from inception until August 28, 2023. Reviews that included RCTs evaluating integrated or stand-alone health app interventions in patient populations with regard to efficacy/effectiveness were considered eligible. Information on indications, outcomes, app characteristics, efficacy/effectiveness results and authors' conclusions was extracted. Methodological quality was assessed using the AMSTAR2 tool. We identified 48 systematic reviews published between 2013 and 2023 (35 with meta-analyses) that met our inclusion criteria. Eleven reviews included a broad spectrum of conditions, thirteen focused on diabetes, five on anxiety and/or depression, and others on various other indications. Reported outcomes ranged from medication adherence to laboratory, anthropometric and functional parameters, symptom scores and quality of life. Fourty-one reviews concluded that health apps may be effective in improving health outcomes. We rated one review as moderate quality. Here we report that the synthesized evidence on health app effectiveness varies largely between indications. Future RCTs should consider reporting behavioral (process) outcomes and measures of healthcare resource utilization to provide deeper insights on mechanisms that make health apps effective, and further elucidate their impact on healthcare systems.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Centre for Disease Control. Telehealth in Rural Communities, https://www.cdc.gov/chronicdisease/resources/publications/factsheets/tel... (2022).
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
