

Classification of Acoustic Hearing Preservation After Cochlear Implantation Using Electrocochleography
- PMID: 38105510
- PMCID: PMC10729624
- DOI: 10.1177/23312165231220997
Classification of Acoustic Hearing Preservation After Cochlear Implantation Using Electrocochleography
Abstract
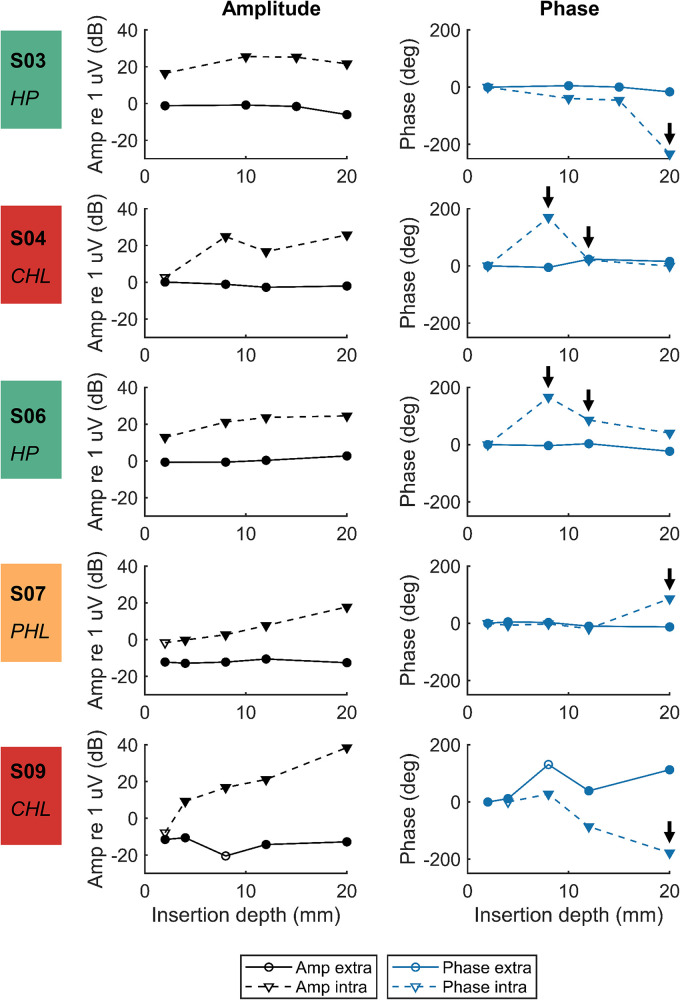
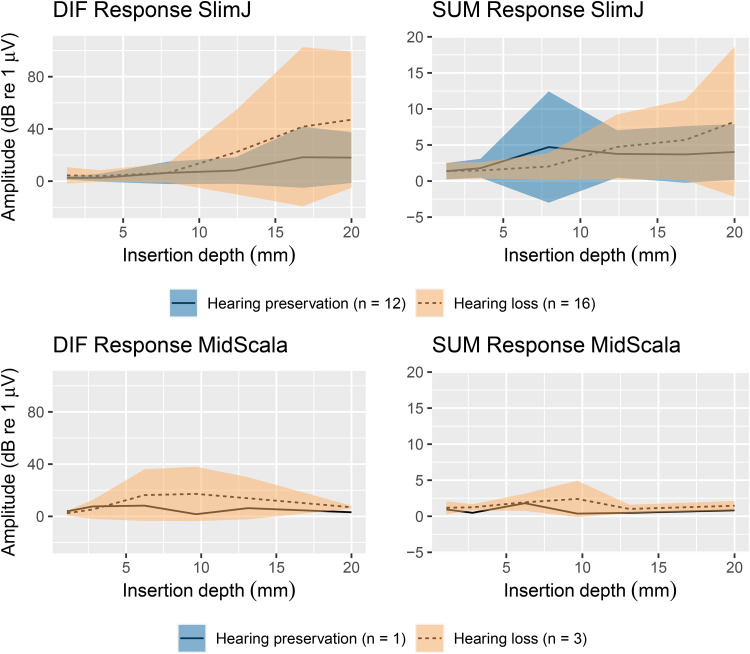
The objective to preserve residual hearing during cochlear implantation has recently led to the use of intracochlear electrocochleography (ECochG) as an intraoperative monitoring tool. Currently, a decrease in the amplitude of the difference between responses to alternating-polarity stimuli (DIF response), predominantly reflecting the hair cell response, is used for providing feedback. Including other ECochG response components, such as phase changes and harmonic distortions, could improve the accuracy of surgical feedback. The objectives of the present study were (1) to compare simultaneously recorded stepwise intracochlear and extracochlear ECochG responses to 500 Hz tone bursts, (2) to explore patterns in features extracted from the intracochlear ECochG recordings relating to hearing preservation or hearing loss, and (3) to design support vector machine (SVM) and random forest (RF) classifiers of acoustic hearing preservation that treat each subject as a sample and use all intracochlear ECochG recordings made during electrode array insertion for classification. Forty subjects undergoing cochlear implant (CI) surgery at the Oslo University Hospital, St. Thomas' Hearing Implant Centre, or the University Hospital of Zurich were prospectively enrolled. In this cohort, DIF response amplitude decreases did not relate to postoperative acoustic hearing preservation. Exploratory analysis of the feature set extracted from the ECochG responses and preoperative audiogram showed that the features were not discriminative between outcome classes. The SVM and RF classifiers that were trained on these features could not distinguish cases with hearing loss and hearing preservation. These findings suggest that hearing loss following CI surgery is not always reflected in intraoperative ECochG recordings.
Keywords: classifier; cochlear implant; electrocochleography; random forest; residual hearing; support vector machine.
Conflict of interest statement
Declaration of Conflicting InterestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures






References
-
- Balkany T. J., Connell S. S., Hodges A. V., Payne S. L., Telischi F. F., Eshraghi A. A., Angeli S. I., Germani R., Messiah S., Arheart K. L. (2006). Conservation of residual acoustic hearing after cochlear implantation. Otology & Neurotology, 27(8), 1083–1088. 10.1097/01.aud.0000444781.15858.f1 - DOI - PubMed
-
- Bester C., Collins A., Razmovski T., Weder S., Briggs R. J., Wei B., Zakaria A. F., Gerard J.-M., Mitchell-Innes A., Tykocinski M., Kennedy R., Iseli C., Dahm M., Ellul S., O'Leary S. (2021). Electrocochleography triggered intervention successfully preserves residual hearing during cochlear implantation: Results of a randomised clinical trial. Hearing Research, 426, 108353. 10.1016/j.heares.2021.108353 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
