

Surveillance for Lyme disease in Canada, 2009-2019
- PMID: 38105769
- PMCID: PMC10723632
- DOI: 10.14745/ccdr.v48i05a05
Surveillance for Lyme disease in Canada, 2009-2019
Abstract
Background: Lyme disease (LD) is a multisystem infection that can affect the skin, heart, joints and nervous system. In Canada, the incidence of LD cases has increased over the past decade making this a disease of public health concern. The objective of this study is to summarize the epidemiology of LD cases reported in Canada from 2009 through 2019.
Methods: Incidence over time, case classification (confirmed and probable), seasonal and geographic distribution, demographic and clinical characteristics of reported LD cases were determined. Logistic regression was used to explore potential demographic risk factors for the occurrence of LD.
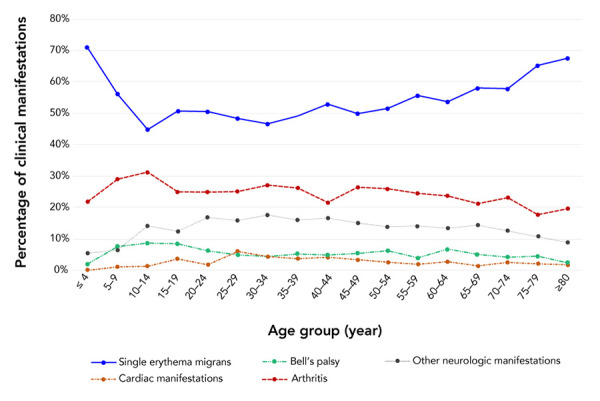
Results: During 2009-2019, a total of 10,150 LD cases were reported by the provinces to the Public Health Agency of Canada, of which 7,242 (71.3%) were confirmed and 2,908 (28.7%) were probable cases. The annual count increased from 144 in 2009 to 2,634 in 2019, mainly due to an increase in locally acquired infections, from 65.3% to 93.6%, respectively. The majority of cases (92.1%) were reported from three provinces: Ontario (46.0%); Nova Scotia (28.0%); and Québec (18.1%). Most of the locally acquired cases (74.0%) were reported in the summer months of June (20.0%), July (35.4%) and August (18.6%). The highest incidence rates (cases per 100,000 population) were in children aged 5-9 years (45.0) and in adults aged 65-69 years (74.3), with 57.3% of all reported cases occurring among males. The most common presenting symptoms were single erythema migrans rash (75.1%) and arthritis (34.1%). The frequency of reported clinical manifestations varied among age groups and seasons with erythema migrans and arthritis at presentation reported more frequently in children than older patients.
Conclusion: The results of this report highlight the continued emergence of LD in Canada and the need for further development and implementation of targeted awareness campaigns designed to minimize the burden of LD.
Keywords: Canada; Ixodes pacificus; Ixodes scapularis; Lyme disease; surveillance; tick-borne disease.
Public Health Agency of Canada, 2022.
Conflict of interest statement
Competing interests None.
Figures




References
-
- Public Health Agency of Canada. Lyme disease surveillance report: Preliminary annual report 2018. Ottawa (ON): PHAC; 2021 (accessed 2021-02-22). https://www.canada.ca/en/public-health/services/publications/diseases-co...
-
- Wormser GP, Dattwyler RJ, Shapiro ED, Halperin JJ, Steere AC, Klempner MS, Krause PJ, Bakken JS, Strle F, Stanek G, Bockenstedt L, Fish D, Dumler JS, Nadelman RB. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2006;43(9):1089–134. 10.1086/508667 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
