

Facial Asymmetry-Demystifying the Entity
- PMID: 38105863
- PMCID: PMC10719165
- DOI: 10.1007/s12663-023-02053-9
Facial Asymmetry-Demystifying the Entity
Abstract
Introduction/background: Perfect facial symmetry has always been considered a hallmark of beauty, but, is almost elusive in nature. However, clinically evident skeletal facial asymmetry on the other hand is quite common, which can result from congenital deformities, developmental abnormalities, secondary to maxillofacial trauma and it is an entity maxillofacial surgeons deal with on a regular basis. Surgical correction of facial asymmetry is challenging, as it not only involves the correction of the skeletal asymmetry for an aesthetic outcome, but, also the improvement of the soft tissue drape and dental occlusal harmony. This results in rehabilitation of functional components of orofacial complex like speech, deglutition and phonation.
Objective: With this paper, we intend to throw a light on this challenging aspect of maxillofacial surgery, along with giving the next generation of maxillofacial surgeons a direction to explore the topic further.
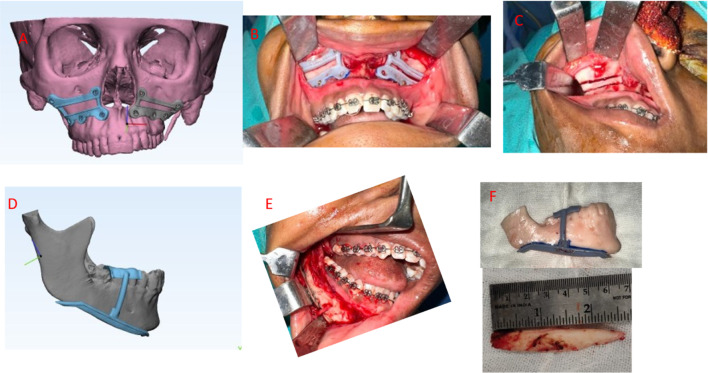
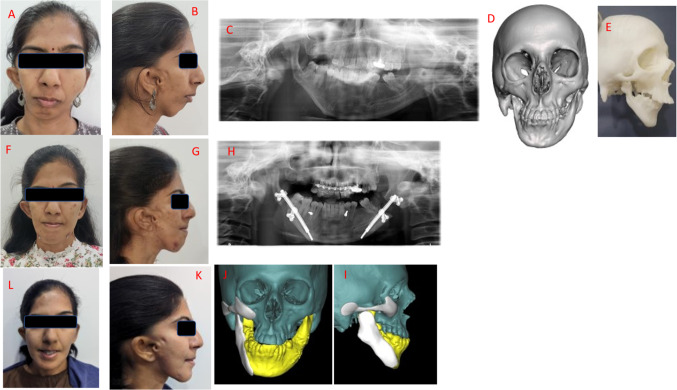
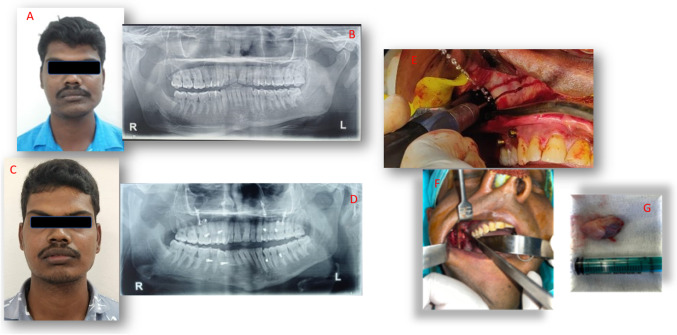
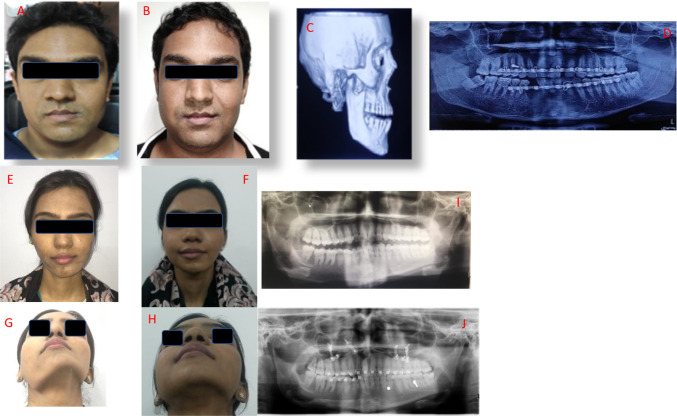
Conclusion: Meticulous evaluation and diagnosis of the patient's problems with latest diagnostic methods like 3-dimensional imaging and surgical treatment with orthognathic surgery, gap arthroplasty or distraction osteogenesis, utilizing cutting edge 3-D virtual planning will result in better outcomes.This review will collate the information available in the literature, along with the authors' recommendations for better planning and execution of this challenging puzzle of facial asymmetry.
Keywords: 3-D virtual planning; Facial asymmetry; Orthognathic surgery; Soft tissue augmentation.
© The Association of Oral and Maxillofacial Surgeons of India 2023. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Figures





References
-
- Cheong YW, Lo LJ. Facial asymmetry: etiology, evaluation, and management. Chang Gung Med J. 2011;34(4):341–351. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous