

Real-Time Acute Kidney Injury Risk Stratification-Biomarker Directed Fluid Management Improves Outcomes in Critically Ill Children and Young Adults
- PMID: 38106571
- PMCID: PMC10719644
- DOI: 10.1016/j.ekir.2023.09.019
Real-Time Acute Kidney Injury Risk Stratification-Biomarker Directed Fluid Management Improves Outcomes in Critically Ill Children and Young Adults
Abstract
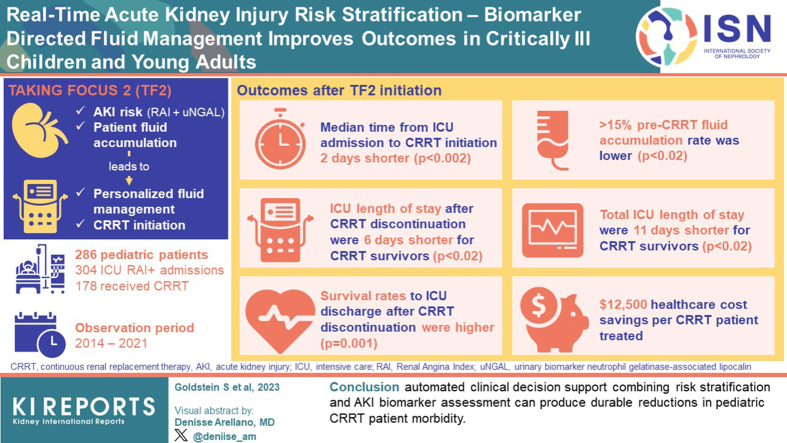
Introduction: Critically ill admitted patients are at high risk of acute kidney injury (AKI). The renal angina index (RAI) and urinary biomarker neutrophil gelatinase-associated lipocalin (uNGAL) can aid in AKI risk assessment. We implemented the Trial in AKI using NGAL and Fluid Overload to optimize CRRT Use (TAKING FOCUS 2; TF2) to personalize fluid management and continuous renal replacement therapy (CRRT) initiation based on AKI risk and patient fluid accumulation. We compared outcomes pre-TF2 and post-TF2 initiation.
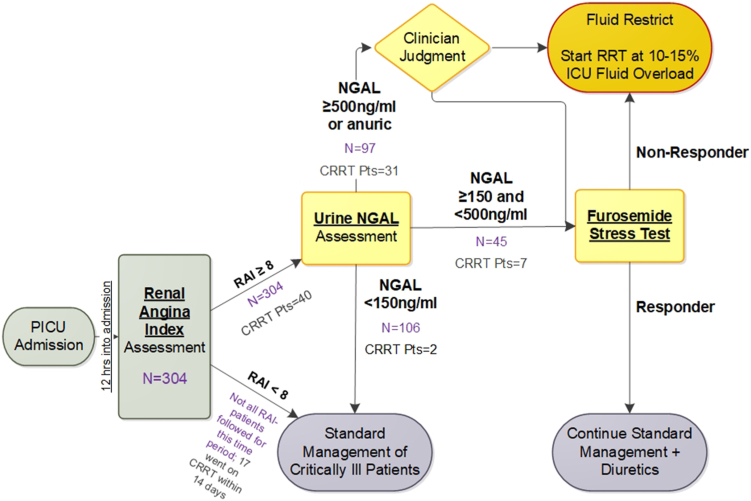
Methods: Patients admitted from July 2017 were followed-up prospectively with the following: (i) an automated RAI result at 12 hours of admission, (ii) a conditional uNGAL order for RAI ≥8, and (iii) a CRRT initiation goal at 10% to 15% weight-based fluid accumulation.
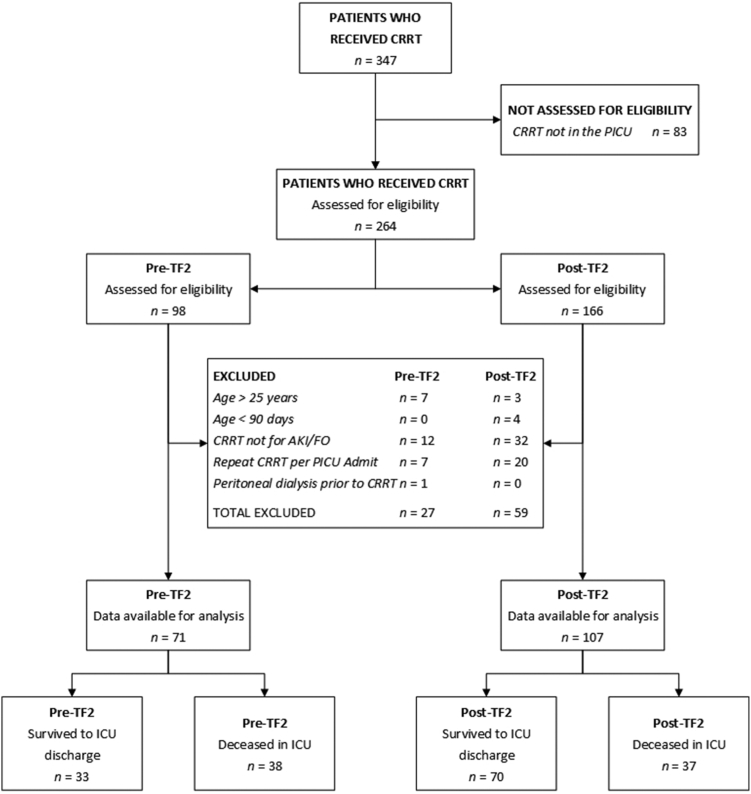
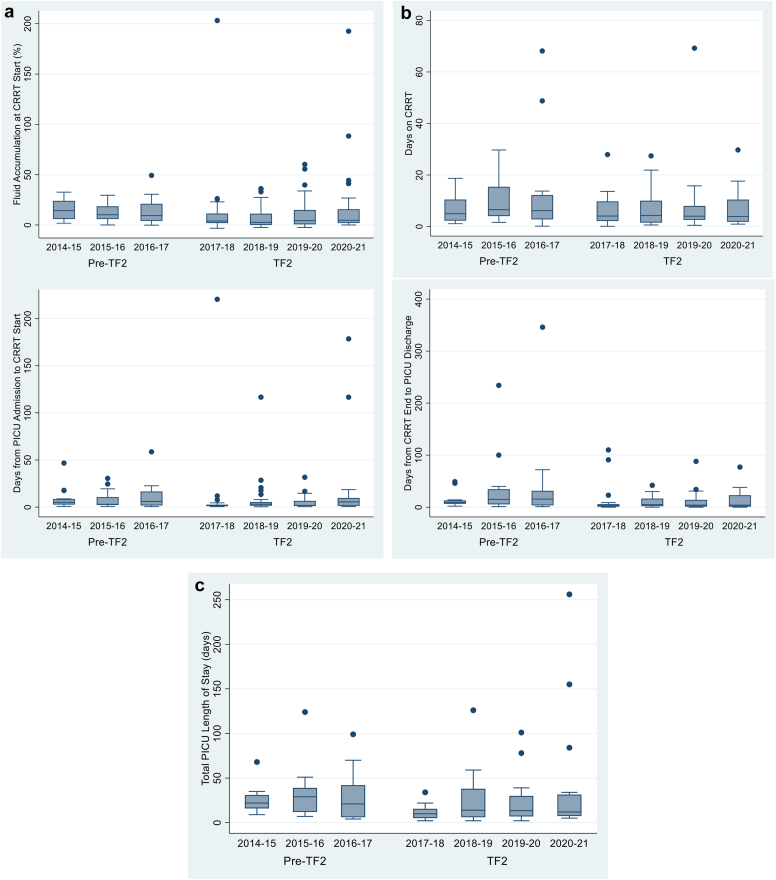
Results: A total of 286 patients comprised 304 intensive care unit (ICU) RAI+ admissions; 178 patients received CRRT over the observation period (2014-2021). Median time from ICU admission to CRRT initiation was 2 days shorter (P < 0.002), and ≥15% pre-CRRT fluid accumulation rate was lower in the TF2 era (P < 0.02). TF2 ICU length of stay (LOS) after CRRT discontinuation and total ICU LOS were 6 and 11 days shorter for CRRT survivors (both P < 0.02). Survival rates to ICU discharge after CRRT discontinuation were higher in the TF2 era (P = 0.001). These associations persisted in each TF2 year; we estimate a conservative $12,500 health care cost savings per CRRT patient treated after TF2 implementation.
Conclusion: We suggest that automated clinical decision support (CDS) combining risk stratification and AKI biomarker assessment can produce durable reductions in pediatric CRRT patient morbidity.
Keywords: acute kidney injury; children; continuous renal replacement therapy; neutrophil gelatinase associated lipocalin; renal angina index.
© 2023 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group KDIGO clinical practice guideline for acute kidney injury. Kidney Interational. 2012;2(suppl 1):1–138.
-
- Schneider J., Khemani R., Grushkin C., Bart R. Serum creatinine as stratified in the RIFLE score for acute kidney injury is associated with mortality and length of stay for children in the pediatric intensive care unit. Crit Care Med. 2010;38:933–939. doi: 10.1097/CCM.0b013e3181cd12e1. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
