

Dorsal Wrist Carpal Boss Impingement-Dynamic Ultrasound to the Rescue!
- PMID: 38106849
- PMCID: PMC10723960
- DOI: 10.1055/s-0043-1772691
Dorsal Wrist Carpal Boss Impingement-Dynamic Ultrasound to the Rescue!
Abstract
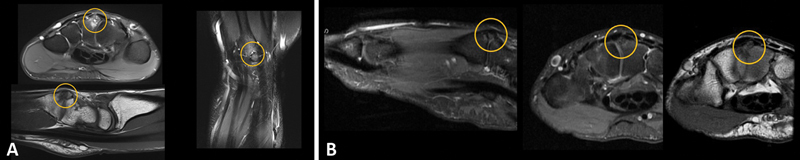
The "carpal boss" is a variant present in 19% of the population according to cadaveric studies but becomes symptomatic in only 1% of cases. With the rising popularity of "yoga," which includes prolonged hyperextension at the wrist joint with weight bearing, an increasing number of individuals with silent carpal boss present with dorsal wrist pain due to impingement over the dorsal soft tissues by this innocuous bony protuberance. This warrants the attention of radiologists and clinicians while dealing with wrist pain. It can be challenging to identify this bossing on routine radiographs, necessitating special views. We describe the use of dynamic ultrasound in diagnosing "symptomatic" carpal boss, the effects of which become even more evident on imaging during hyperextension-the triggering movement.
Keywords: carpal boss; dynamic ultrasound; impingement.
Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures





References
-
- Porrino J, Maloney E, Chew F S. Current concepts of the carpal boss: pathophysiology, symptoms, clinical or imaging diagnosis, and management. Curr Probl Diagn Radiol. 2015;44(05):462–468. - PubMed
-
- Clarke A M, Wheen D J, Visvanathan S, Herbert T J, Conolly W B. The symptomatic carpal boss. Is simple excision enough? J Hand Surg [Br] 1999;24(05):591–595. - PubMed
LinkOut - more resources
Full Text Sources