

The Glioblastoma Landscape: Hallmarks of Disease, Therapeutic Resistance, and Treatment Opportunities
- PMID: 38107346
- PMCID: PMC10723753
- DOI: 10.18103/mra.v11i6.3994
The Glioblastoma Landscape: Hallmarks of Disease, Therapeutic Resistance, and Treatment Opportunities
Abstract
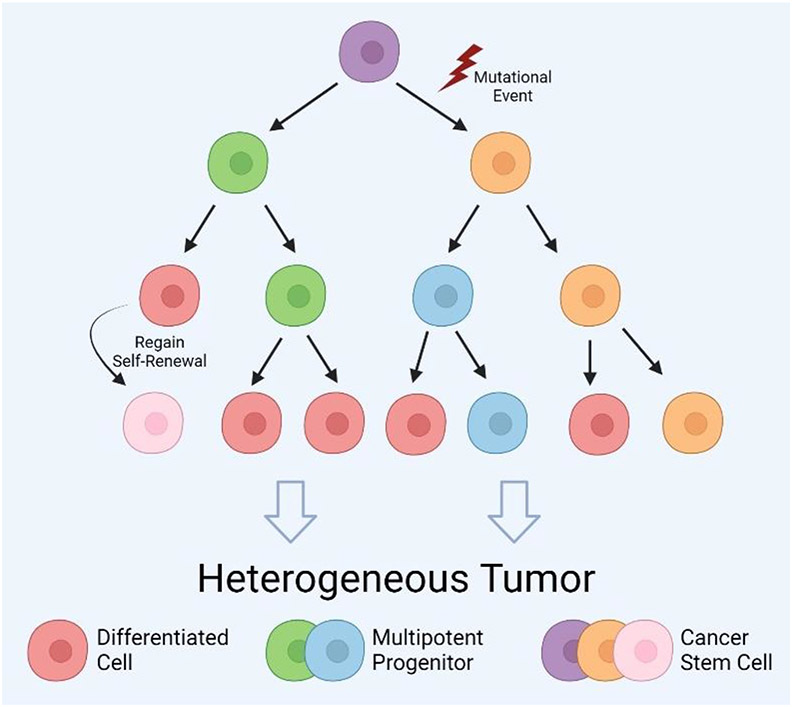
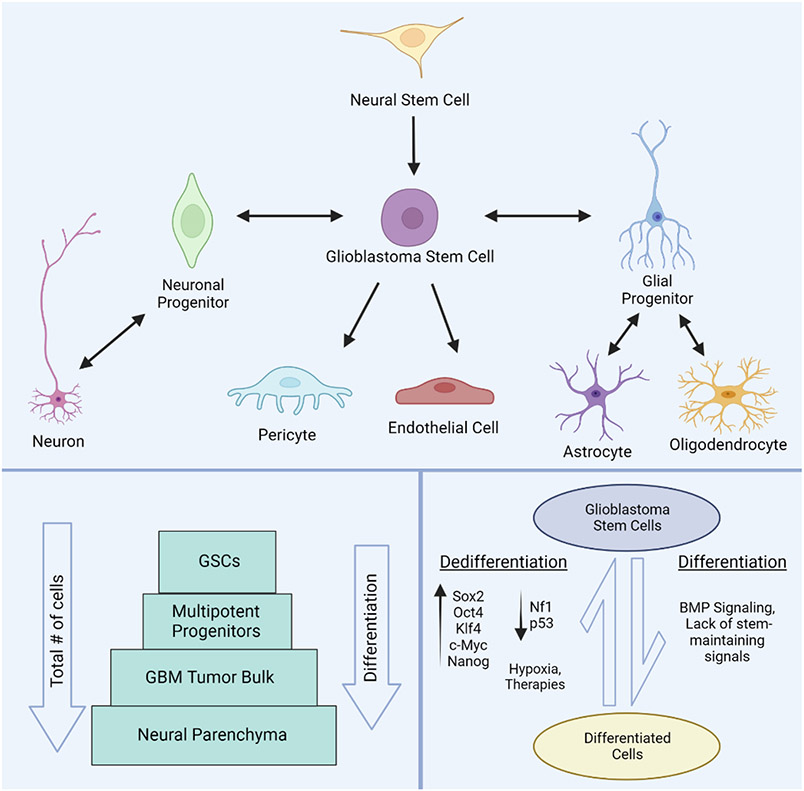
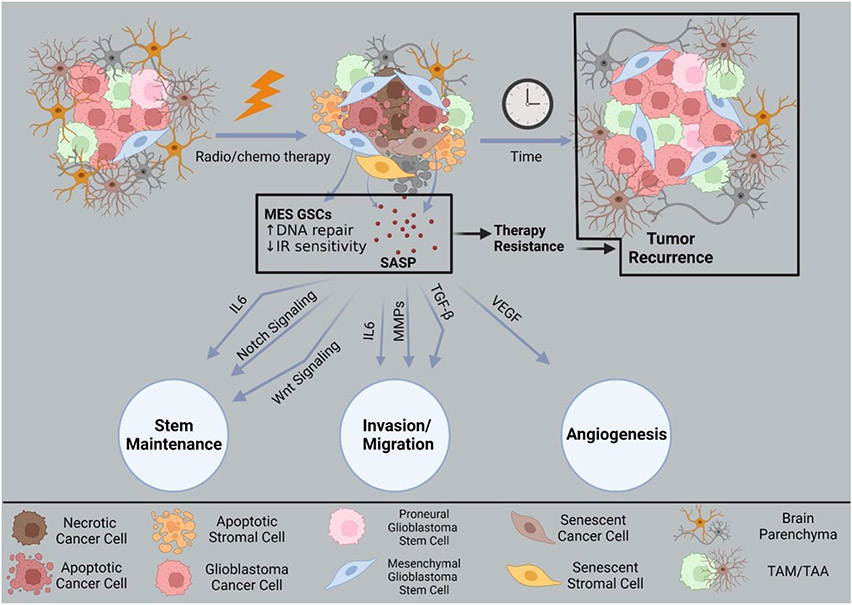
Malignant brain tumors are aggressive and difficult to treat. Glioblastoma is the most common and lethal form of primary brain tumor, often found in patients with no genetic predisposition. The median life expectancy for individuals diagnosed with this condition is 6 months to 2 years and there is no known cure. New paradigms in cancer biology implicate a small subset of tumor cells in initiating and sustaining these incurable brain tumors. Here, we discuss the heterogenous nature of glioblastoma and theories behind its capacity for therapy resistance and recurrence. Within the cancer landscape, cancer stem cells are thought to be both tumor initiators and major contributors to tumor heterogeneity and therapy evasion and such cells have been identified in glioblastoma. At the cellular level, disruptions in the delicate balance between differentiation and self-renewal spur transformation and support tumor growth. While rapidly dividing cells are more sensitive to elimination by traditional treatments, glioblastoma stem cells evade these measures through slow division and reversible exit from the cell cycle. At the molecular level, glioblastoma tumor cells exploit several signaling pathways to evade conventional therapies through improved DNA repair mechanisms and a flexible state of senescence. We examine these common evasion techniques while discussing potential molecular approaches to better target these deadly tumors. Equally important, the presented information encourages the idea of augmenting conventional treatments with novel glioblastoma stem cell-directed therapies, as eliminating these harmful progenitors holds great potential to modulate tumor recurrence.
Keywords: Glioblastoma; Glioblastoma stem cells; clinical treatments; heterogeneity; therapy resistance; tumor microenvironment.
Conflict of interest statement
Conflict of interest statement. The authors have no conflicts of interest to declare.
Figures
References
-
- Rock K, Mcardle O, Forde P, et al. A clinical review of treatment outcomes in glioblastoma multiforme—the validation in a non-trial population of the results of a randomised Phase III clinical trial: has a more radical approach improved survival? Br J Radiol. 2012;85(1017):e729–e733. doi:10.1259/bjr/83796755 - DOI - PMC - PubMed
-
- Schapira AHV. Neurology and Clinical Neuroscience E-Book. Elsevier Health Sciences; 2006
Grants and funding
LinkOut - more resources
Full Text Sources