

Prevalence and characteristics of thelarche variant
- PMID: 38107513
- PMCID: PMC10722224
- DOI: 10.3389/fendo.2023.1303989
Prevalence and characteristics of thelarche variant
Abstract
Introduction: Girls with early thelarche may show an intermediate clinical picture between isolated premature thelarche (PT) and central precocious puberty (CPP), defined as "thelarche variant" (TV), characterized by an FSH-predominant response, although a univocal definition is lacking.
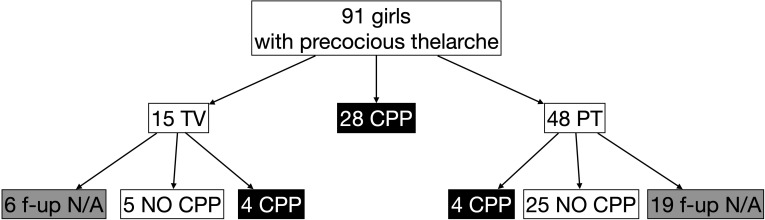
Methods: Retrospective analysis on 91 girls with early thelarche (<8 years) and advanced bone age and/or accelerated growth who underwent 104 LHRH tests. Patients were classified into CPP (LH peak ≥5 IU/L; n = 28, 31%), TV (FSH peak ≥20 IU/L, LH peak <5 IU/L; n = 15, 16%), or PT (FSH peak <20 IU/L and LH peak <5 IU/L; n = 48, 53%).
Results: TV patients were younger (5.51 years) and with less advanced bone age (+0.8 years). They had higher basal and peak FSH (2.5 and 26.6 IU/L) and lower basal and peak LH/FSH ratios (0.08 and 0.11). The prevalence of presence of ovarian follicles >5 mm in TV (42%) was similar to CPP but significantly higher than PT, whereas maximum ovarian volume was smaller in TV (1.0 cm3). At the last follow-up visit (available in 60% of the cases), 44% of TV developed CPP compared with 14% of PT (p = 0.04). At first evaluation, those who progressed to CPP had a higher basal FSH (3.2 IU/L), lower LH/FSH ratio (0.07), and a higher peak LH (4.1 IU/L) compared with those who did not progress to CPP (basal FSH 1.9 IU/L, p < 0.01; basal LH/FSH ratio 0.12, p < 0.01; peak LH 2.8 IU/L, p = 0.02).
Conclusion: Using laboratory parameters only as a definition, we identified the clinical, laboratory, and imaging features of TV: these girls showed less advanced bone age and FSH predominance also at baseline, with smaller ovaries but with follicles >5 mm. Almost half of girls initially diagnosed as TV developed CPP at last follow-up visit, and these girls had higher baseline FSH, lower baseline LH/FSH ratio, and higher peak LH at first evaluation. Therefore, TV may represent a "precocious prepuberty" in which the FSH predominance may initially limit the progression into proper puberty, but it may eventually trigger full puberty (even CPP, depending on the girls' age).
Keywords: FSH & LH; endocrinologic diseases; epidemiology; precocious puberty; stimulation tests; thelarche premature; thelarche variant.
Copyright © 2023 Burlo, Lorenzon, Tamaro, Fabretto, Buonomo, Peinkhofer, Vidonis, Vittori, Faleschini, Barbi and Tornese.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources