

Intravenous Thrombolysis for Acute Ischemic Stroke in Patients With Recent Direct Oral Anticoagulant Use: A Systematic Review and Meta-Analysis
- PMID: 38108256
- PMCID: PMC10863770
- DOI: 10.1161/JAHA.123.031669
Intravenous Thrombolysis for Acute Ischemic Stroke in Patients With Recent Direct Oral Anticoagulant Use: A Systematic Review and Meta-Analysis
Abstract
Background: Intravenous thrombolysis (IVT) is an effective stroke therapy that remains underused. Currently, the use of IVT in patients with recent direct oral anticoagulant (DOAC) intake is not recommended. In this study we aim to investigate the safety and efficacy of IVT in patients with acute ischemic stroke and recent DOAC use.
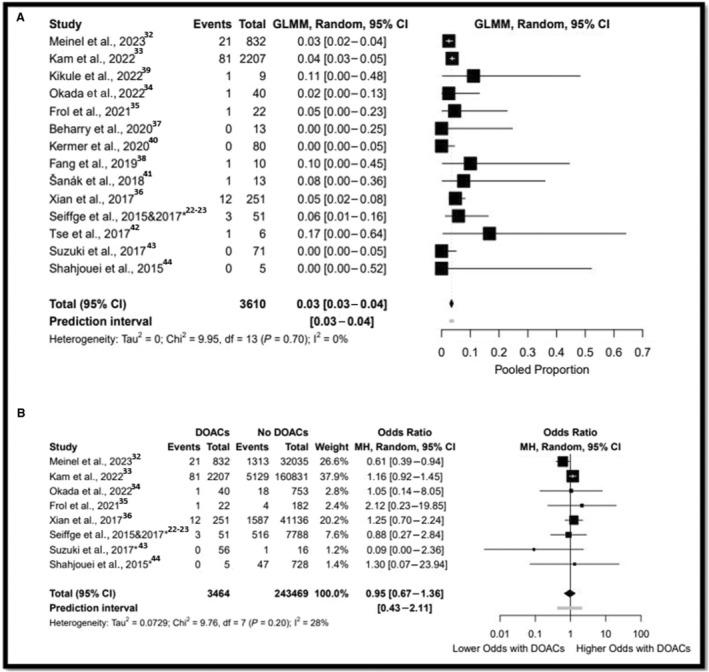
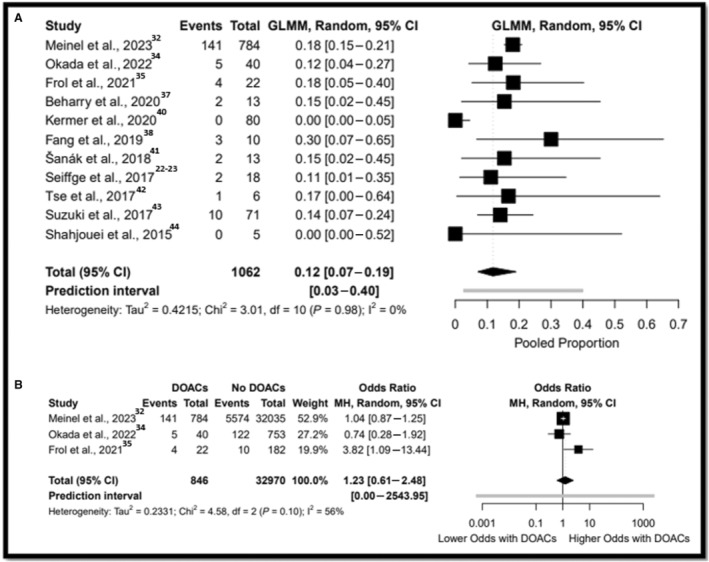
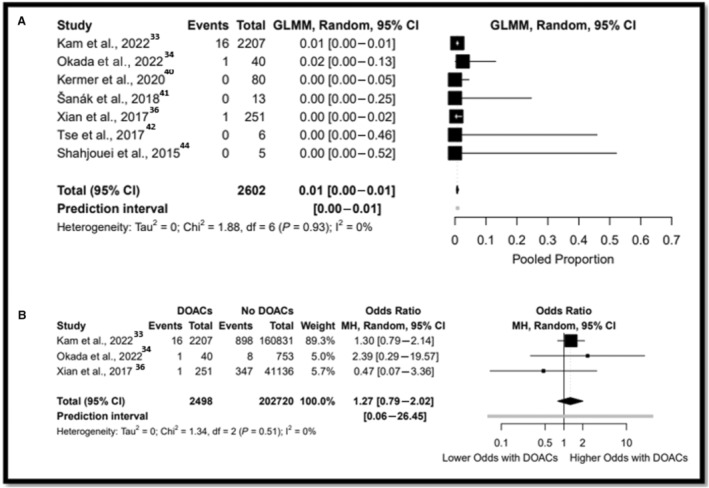
Methods and results: A systematic review and meta-analysis of proportions evaluating IVT with recent DOAC use was conducted. Outcomes included symptomatic intracranial hemorrhage, any intracranial hemorrhage, serious systemic bleeding, and 90-day functional independence (modified Rankin scale score 0-2). Additionally, rates were compared between patients receiving IVT using DOAC and non-DOAC by a random effect meta-analysis to calculate pooled odds ratios (OR) for each outcome. Finally, sensitivity analysis for idarucizumab, National Institutes of Health Stroke Scale, and timing of DOAC administration was completed. Fourteen studies with 247 079 patients were included (3610 in DOAC and 243 469 in non-DOAC). The rates of IVT complications in the DOAC group were 3% (95% CI, 3-4) symptomatic intracranial hemorrhage, 12% (95% CI, 7-19) any ICH, and 0.7% (95%CI, 0-1) serious systemic bleeding, and 90-day functional independence was achieved in 57% (95% CI, 43-70). The rates of symptomatic intracranial hemorrhage (3.4 versus 3.5%; OR, 0.95 [95% CI, 0.67-1.36]), any intracranial hemorrhage (17.7 versus 17.3%; OR, 1.23 [95% CI, 0.61-2.48]), serious systemic bleeding (0.7 versus 0.6%; OR, 1.27 [95% CI, 0.79-2.02]), and 90-day modified Rankin scale score 0-2 (46.4 versus 56.8%; OR, 1.21 [95% CI, 0.400-3.67]) did not differ between DOAC and non-DOAC groups. There was no difference in symptomatic intracranial hemorrhage rate based on idarucizumab administration.
Conclusions: Patients with acute ischemic stroke treated with IVT in recent DOAC versus non-DOAC use have similar rates of hemorrhagic complications and functional independence. Further prospective randomized trials are warranted.
Keywords: acute ischemic stroke; coagulopathy; direct oral anticoagulants; idarucizumab; intravenous thrombolysis; safety; symptomatic intracranial hemorrhage.
Figures
References
-
- Organization WH . The Global Burden of Disease: 2004 Update. World Health Organization; 2008.
-
- Callaly E, Ni Chroinin D, Hannon N, Marnane M, Akijian L, Sheehan O, Merwick A, Hayden D, Horgan G, Duggan J, et al. Rates, predictors, and outcomes of early and late recurrence after stroke: the North Dublin Population Stroke study. Stroke. 2016;47:244–246. doi: 10.1161/STROKEAHA.115.011248 - DOI - PubMed
-
- Perera KS, Vanassche T, Bosch J, Swaminathan B, Mundl H, Giruparajah M, Barboza MA, O'Donnell MJ, Gomez‐Schneider M, Hankey GJ, et al. Global survey of the frequency of atrial fibrillation‐associated stroke: embolic stroke of undetermined source global registry. Stroke. 2016;47:2197–2202. doi: 10.1161/STROKEAHA.116.013378 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
