

Genetic and epigenetic features of bilateral Wilms tumor predisposition in patients from the Children's Oncology Group AREN18B5-Q
- PMID: 38110397
- PMCID: PMC10728430
- DOI: 10.1038/s41467-023-43730-0
Genetic and epigenetic features of bilateral Wilms tumor predisposition in patients from the Children's Oncology Group AREN18B5-Q
Abstract
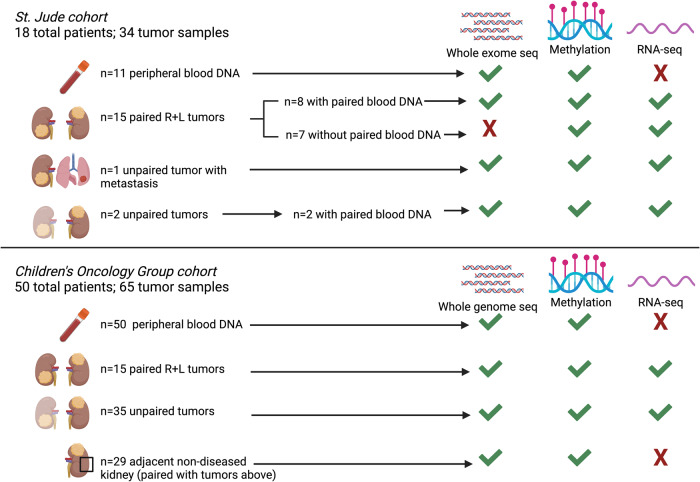
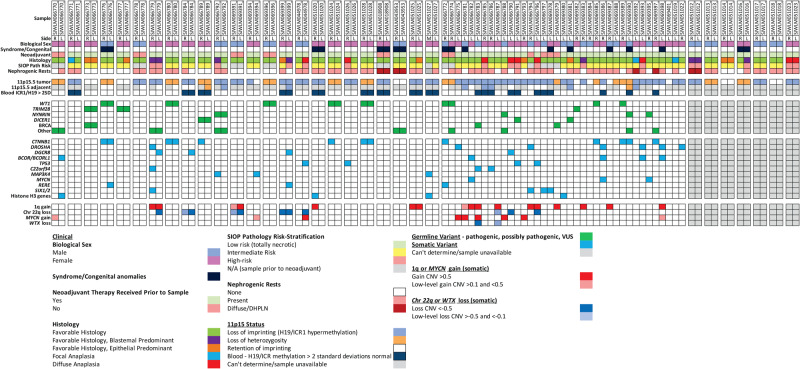
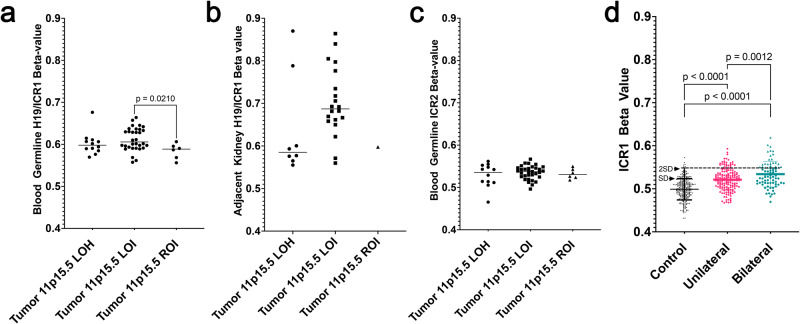
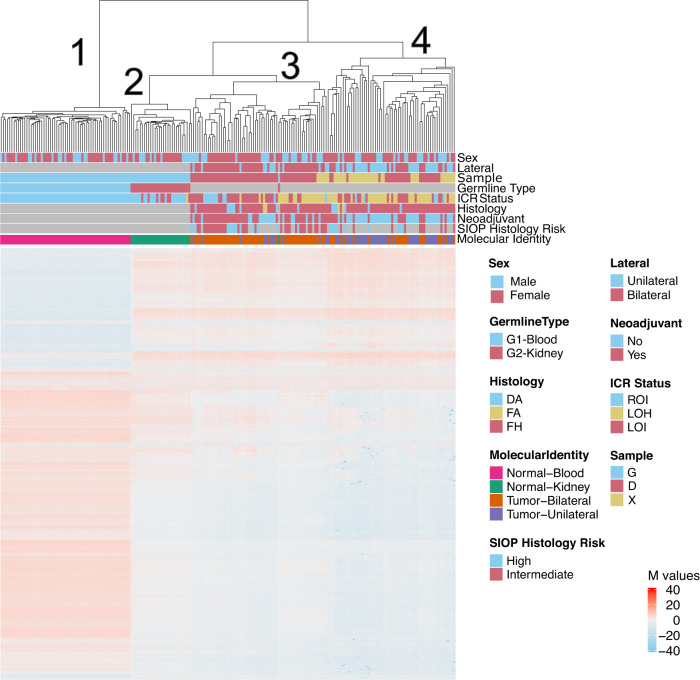
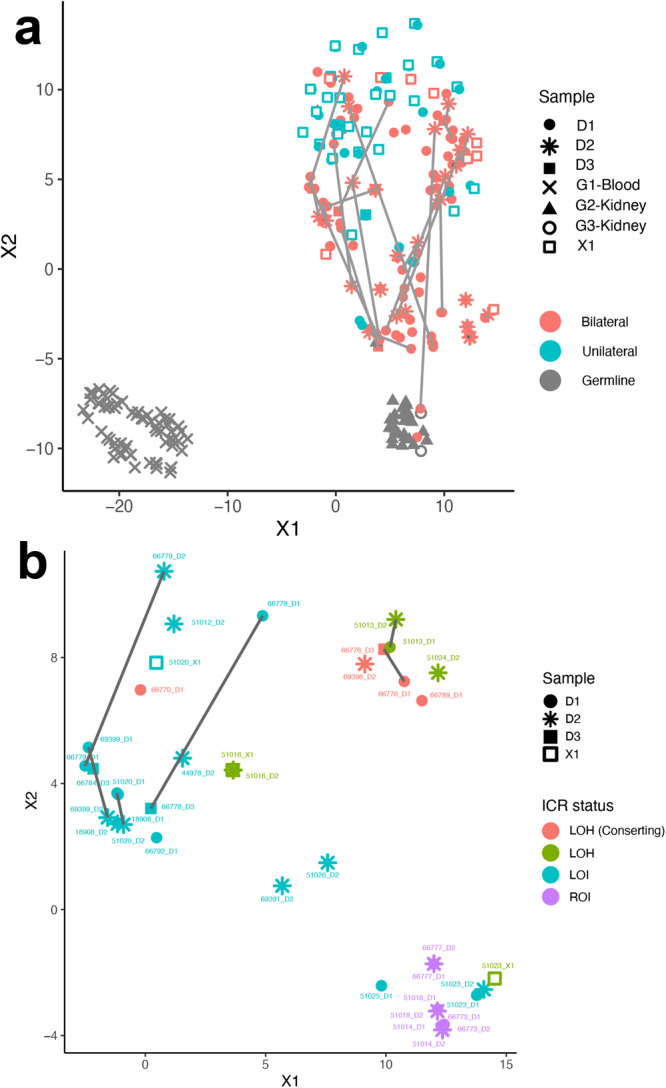
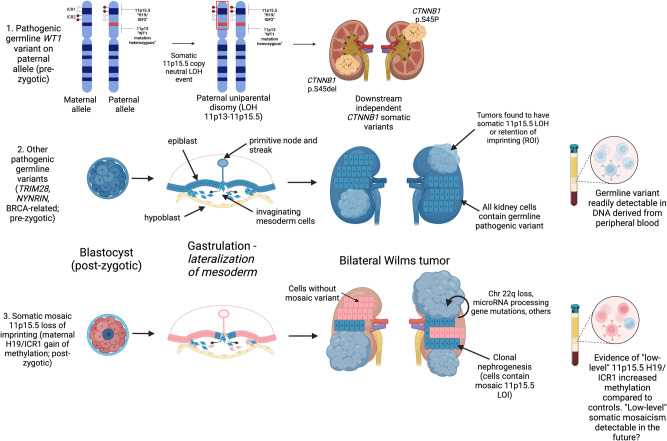
Developing synchronous bilateral Wilms tumor suggests an underlying (epi)genetic predisposition. Here, we evaluate this predisposition in 68 patients using whole exome or genome sequencing (n = 85 tumors from 61 patients with matched germline blood DNA), RNA-seq (n = 99 tumors), and DNA methylation analysis (n = 61 peripheral blood, n = 29 non-diseased kidney, n = 99 tumors). We determine the predominant events for bilateral Wilms tumor predisposition: 1)pre-zygotic germline genetic variants readily detectable in blood DNA [WT1 (14.8%), NYNRIN (6.6%), TRIM28 (5%), and BRCA-related genes (5%)] or 2)post-zygotic epigenetic hypermethylation at 11p15.5 H19/ICR1 that may require analysis of multiple tissue types for diagnosis. Of 99 total tumor specimens, 16 (16.1%) have 11p15.5 normal retention of imprinting, 25 (25.2%) have 11p15.5 copy neutral loss of heterozygosity, and 58 (58.6%) have 11p15.5 H19/ICR1 epigenetic hypermethylation (loss of imprinting). Here, we ascertain the epigenetic and genetic modes of bilateral Wilms tumor predisposition.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
The Genetic and Epigenetic Features of Bilateral Wilms Tumor Predisposition: A Report from the Children's Oncology Group AREN18B5-Q Study.Res Sq [Preprint]. 2023 Mar 16:rs.3.rs-2675436. doi: 10.21203/rs.3.rs-2675436/v1. Res Sq. 2023. Update in: Nat Commun. 2023 Dec 18;14(1):8006. doi: 10.1038/s41467-023-43730-0. PMID: 36993649 Free PMC article. Updated. Preprint.
References
-
- Knudson AG, Strong LC. Mutation and cancer: A model for Wilms’ tumor of the kidney. J. Natl. Cancer Inst. 1972;48:313–24. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
