

Refining the diagnosis of gestational diabetes mellitus: a systematic review and meta-analysis
- PMID: 38110524
- PMCID: PMC10728189
- DOI: 10.1038/s43856-023-00393-8
Refining the diagnosis of gestational diabetes mellitus: a systematic review and meta-analysis
Abstract
Background: Perinatal outcomes vary for women with gestational diabetes mellitus (GDM). The precise factors beyond glycemic status that may refine GDM diagnosis remain unclear. We conducted a systematic review and meta-analysis of potential precision markers for GDM.
Methods: Systematic literature searches were performed in PubMed and EMBASE from inception to March 2022 for studies comparing perinatal outcomes among women with GDM. We searched for precision markers in the following categories: maternal anthropometrics, clinical/sociocultural factors, non-glycemic biochemical markers, genetics/genomics or other -omics, and fetal biometry. We conducted post-hoc meta-analyses of a subset of studies with data on the association of maternal body mass index (BMI, kg/m2) with offspring macrosomia or large-for-gestational age (LGA).
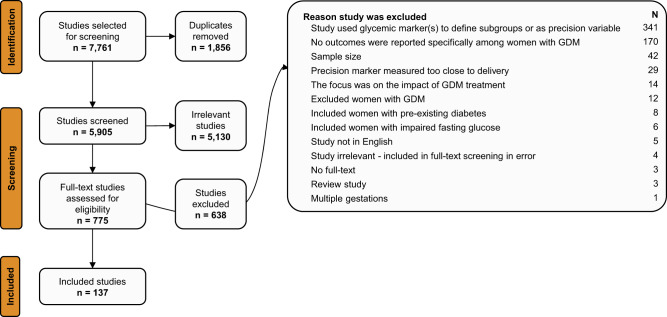
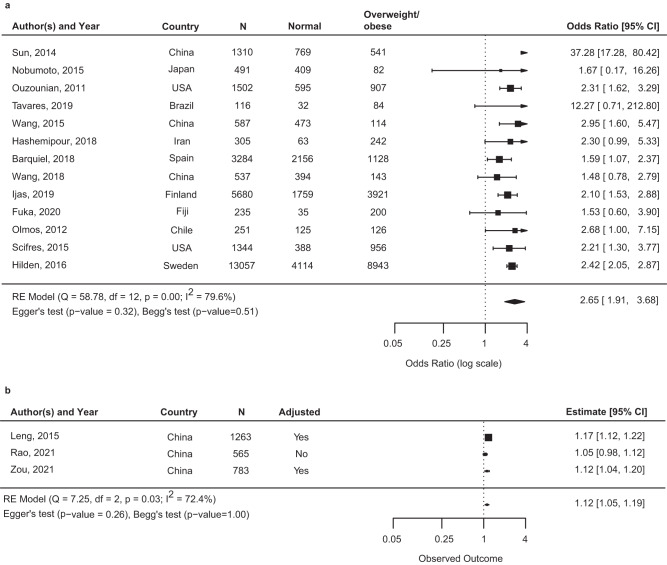
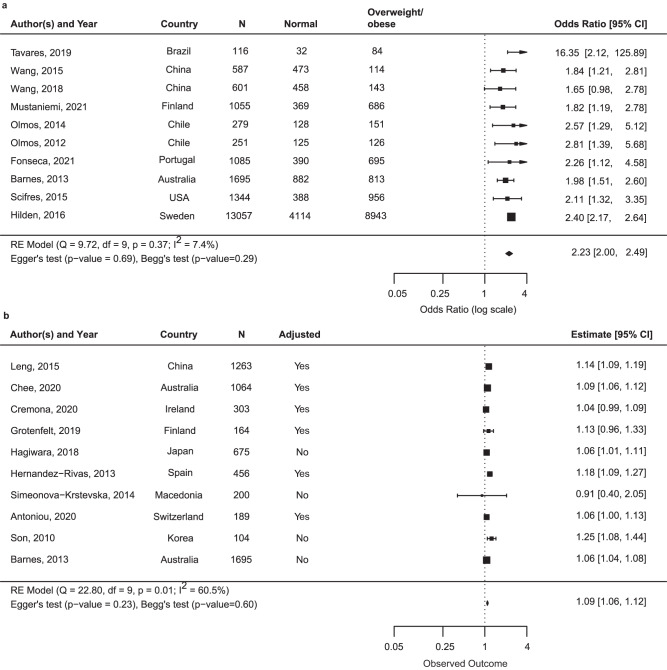
Results: A total of 5905 titles/abstracts were screened, 775 full-texts reviewed, and 137 studies synthesized. Maternal anthropometrics were the most frequent risk marker. Meta-analysis demonstrated that women with GDM and overweight/obesity vs. GDM with normal range BMI are at higher risk of offspring macrosomia (13 studies [n = 28,763]; odds ratio [OR] 2.65; 95% Confidence Interval [CI] 1.91, 3.68), and LGA (10 studies [n = 20,070]; OR 2.23; 95% CI 2.00, 2.49). Lipids and insulin resistance/secretion indices were the most studied non-glycemic biochemical markers, with increased triglycerides and insulin resistance generally associated with greater risk of offspring macrosomia or LGA. Studies evaluating other markers had inconsistent findings as to whether they could be used as precision markers.
Conclusions: Maternal overweight/obesity is associated with greater risk of offspring macrosomia or LGA in women with GDM. Pregnancy insulin resistance or hypertriglyceridemia may be useful in GDM risk stratification. Future studies examining non-glycemic biochemical, genetic, other -omic, or sociocultural precision markers among women with GDM are warranted.
Plain language summary
Gestational Diabetes (GDM) is high blood sugar that develops during pregnancy and may cause complications. GDM diagnosis is centered on blood sugar levels. Despite everyone receiving standard treatment, the clinical outcomes may vary from one individual to another. This indicates a need to identify factors that may help GDM diagnosis and result in improved classification of those at greatest risk for complications. Here, we systematically analyzed all published evidence for potential markers that could identify those with GDM who have greater risk of complications. We find that high maternal weight is a risk factor for offspring born larger for their gestational age. Other promising markers were identified, but further analysis is needed before they can be applied in the clinic.
© 2023. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: C.E.P. is an Associate Editor of Diabetes Care, receives payments from Wolters Kluwer for UpToDate chapters on diabetes in pregnancy, and has received payments for consulting and speaking from Mediflix Inc. All other authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
