

Case series of branch retinal vein occlusion secondary to rhegmatogenous retinal detachment and its surgical management
- PMID: 38110856
- PMCID: PMC10729475
- DOI: 10.1186/s12886-023-03244-1
Case series of branch retinal vein occlusion secondary to rhegmatogenous retinal detachment and its surgical management
Abstract
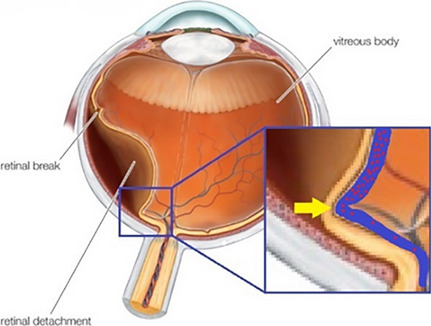
Background: To review cases of branch retinal vein occlusion (BRVO) secondary to rhegmatogenous retinal detachment (RRD) and its surgical management and presume their mechanism.
Methods: Medical records of patients who underwent surgery for RRD between 2015 and 2019 at a single tertiary care center were retrospectively reviewed. New BRVO secondary to RRD or its surgical procedure was diagnosed based on the fundus examination and its clinical course.
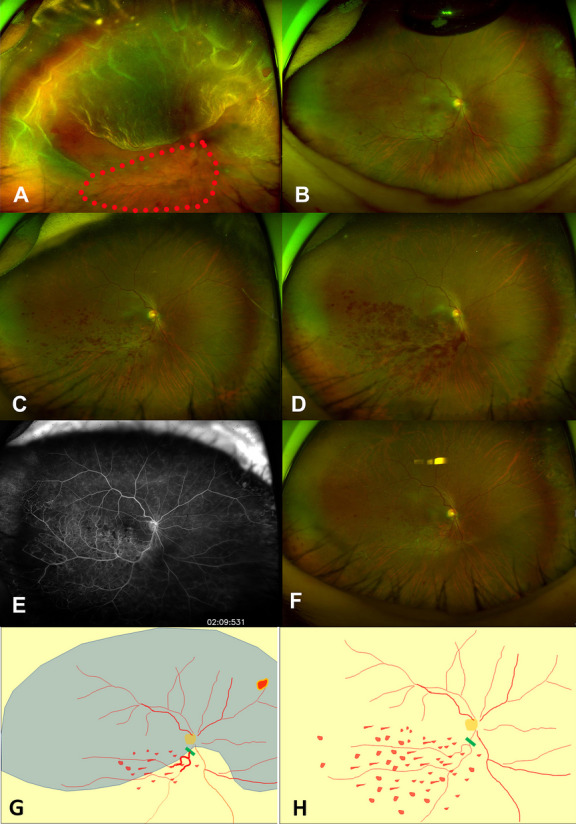
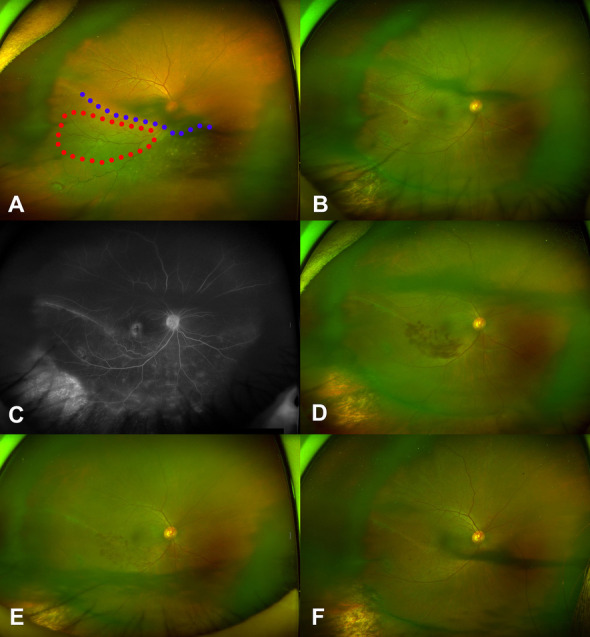
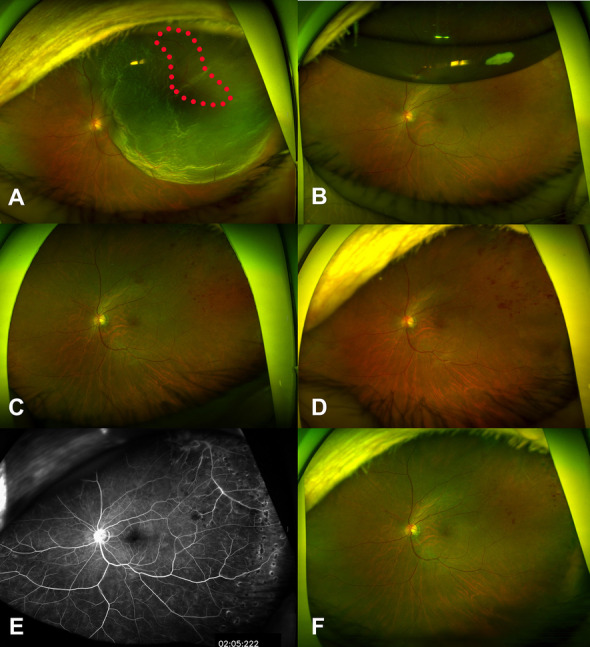
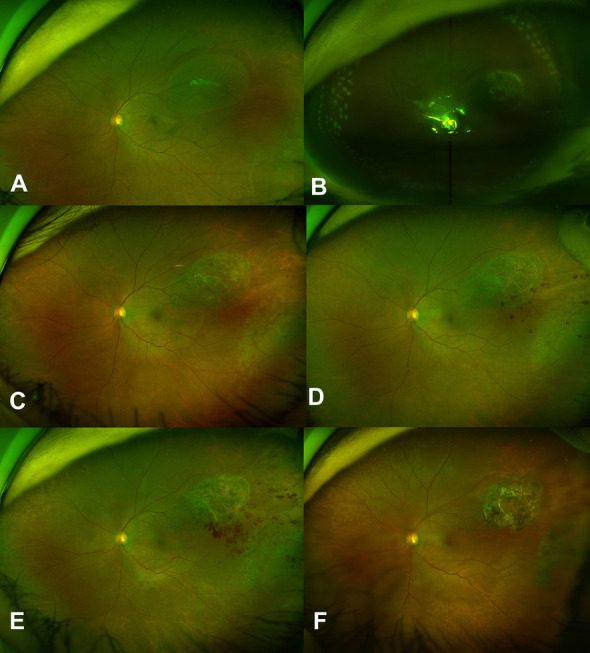
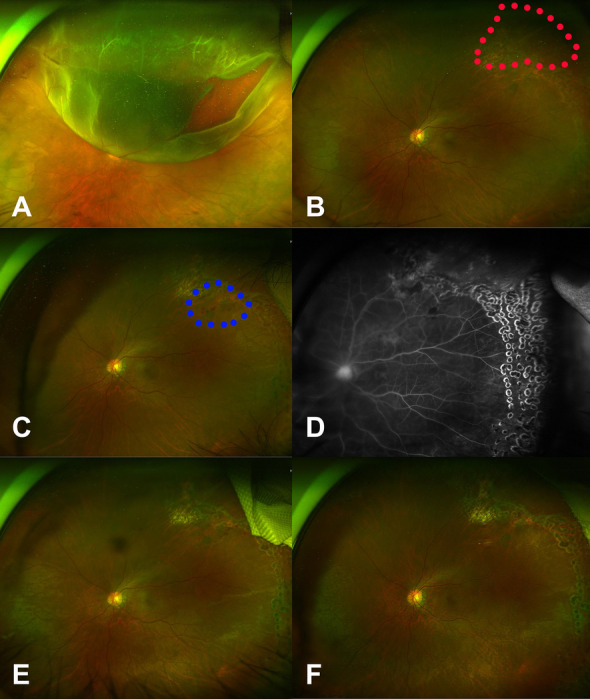
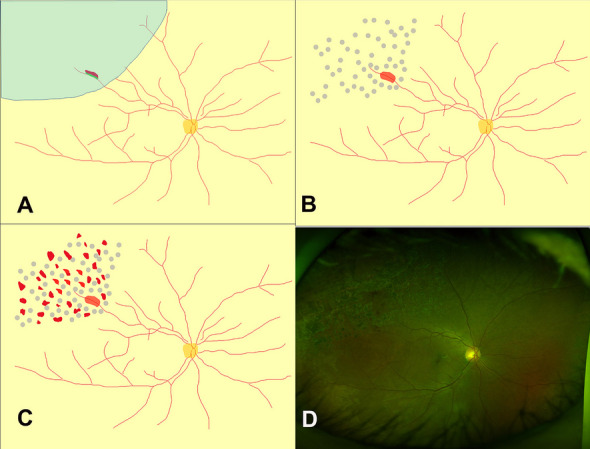
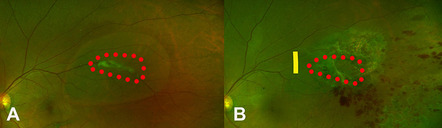
Results: A total of 734 RRD surgeries were performed for five years, and six cases of new BRVOs were noticed in the first year after surgery (incidence was 0.68%: six cases of BRVO / 734 cases of surgical RRD); five cases occurred after vitrectomy, and one occurred after scleral buckling. In three cases, retinal veins were presumed to already be partially occluded related due to a kink of the retinal vein seen before surgery. In the other three cases, the retinal veins were presumed to have incurred damage during vitrectomy.
Conclusion: In the present cohort, RRD or its related procedures caused BRVO within a year of surgery at an incidence of 0.68%. The proposed mechanisms are kinks of the retinal vein on the detached retina and damage to the retinal vein during vitrectomy.
Keywords: Branch retinal vein occlusion; Complication; Rhegmatogenous retinal detachment; Scleral buckling; Vitrectomy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Retinal breaks and rhegmatogenous retinal detachment in association with branch retinal vein occlusion.Ophthalmic Surg Lasers. 1999 Apr;30(4):285-8. Ophthalmic Surg Lasers. 1999. PMID: 10219032
-
Retinal detachment after branch retinal vein occlusion: influence of the type of break on the outcome of vitreous surgery.Ophthalmology. 1997 Jan;104(1):27-32. doi: 10.1016/s0161-6420(97)30366-2. Ophthalmology. 1997. PMID: 9022100
-
Scleral buckling versus vitrectomy for young japanese patients with rhegmatogenous retinal detachment in the era of microincision surgery: real-world evidence from a multicentre study in Japan.Acta Ophthalmol. 2019 Aug;97(5):e736-e741. doi: 10.1111/aos.14050. Epub 2019 Feb 11. Acta Ophthalmol. 2019. PMID: 30741467
-
Pars plana vitrectomy versus scleral buckling for repairing simple rhegmatogenous retinal detachments.Cochrane Database Syst Rev. 2019 Mar 8;3(3):CD009562. doi: 10.1002/14651858.CD009562.pub2. Cochrane Database Syst Rev. 2019. PMID: 30848830 Free PMC article.
-
Rhegmatogenous retinal detachment surgery: A review.Clin Exp Ophthalmol. 2023 Apr;51(3):271-279. doi: 10.1111/ceo.14205. Epub 2023 Jan 25. Clin Exp Ophthalmol. 2023. PMID: 36640144 Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
