

Pancreas CT assessment for pancreatic ductal adenocarcinoma resectability: effect of tube voltage and slice thickness on image quality and diagnostic performance
- PMID: 38111054
- PMCID: PMC10729459
- DOI: 10.1186/s40644-023-00637-9
Pancreas CT assessment for pancreatic ductal adenocarcinoma resectability: effect of tube voltage and slice thickness on image quality and diagnostic performance
Abstract
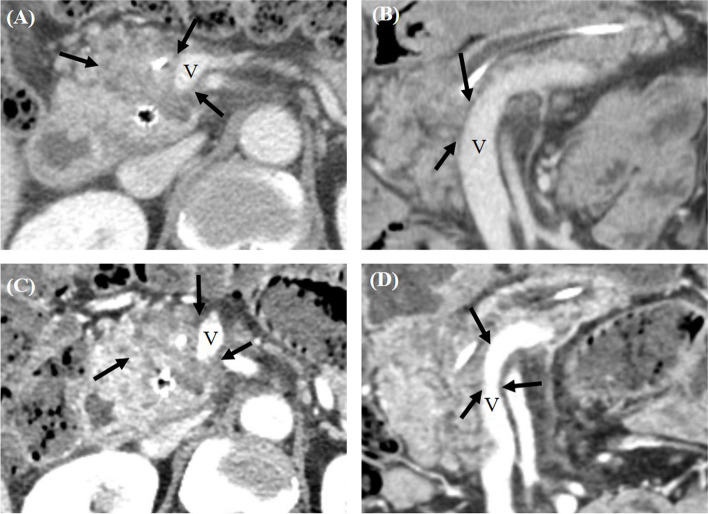
Objectives: To assess the resectability of pancreatic ductal adenocarcinoma (PDAC), the evaluation of tumor vascular contact holds paramount significance. This study aimed to compare the image quality and diagnostic performance of high-resolution (HR) pancreas computed tomography (CT) using an 80 kVp tube voltage and a thin slice (1 mm) for assessing PDAC resectability, in comparison with the standard protocol CT using 120 kVp.
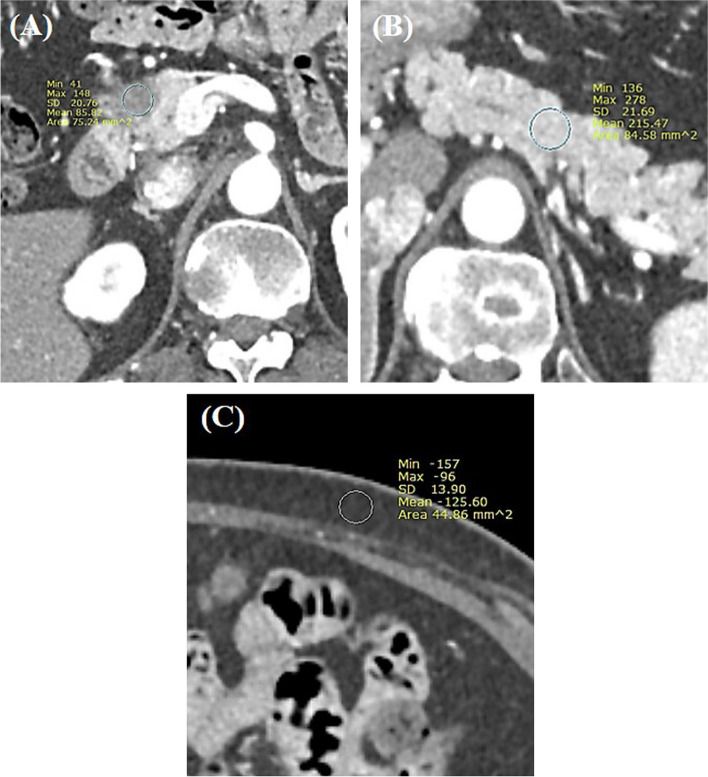
Methods: This research constitutes a secondary analysis originating from a multicenter prospective study. All participants underwent both the standard protocol pancreas CT using 120 kVp with 3 mm slice thickness (ST) and HR-CT utilizing an 80 kVp tube voltage and 1 mm ST. The contrast-to-noise ratio (CNR) between parenchyma and tumor, along with the degree of enhancement of the abdominal aorta and main portal vein (MPV), were measured and subsequently compared. Additionally, the likelihood of margin-negative resection (R0) was evaluated using a five-point scale. The diagnostic performance of both CT protocols in predicting R0 resection was assessed through the area under the receiver operating characteristic curve (AUC).
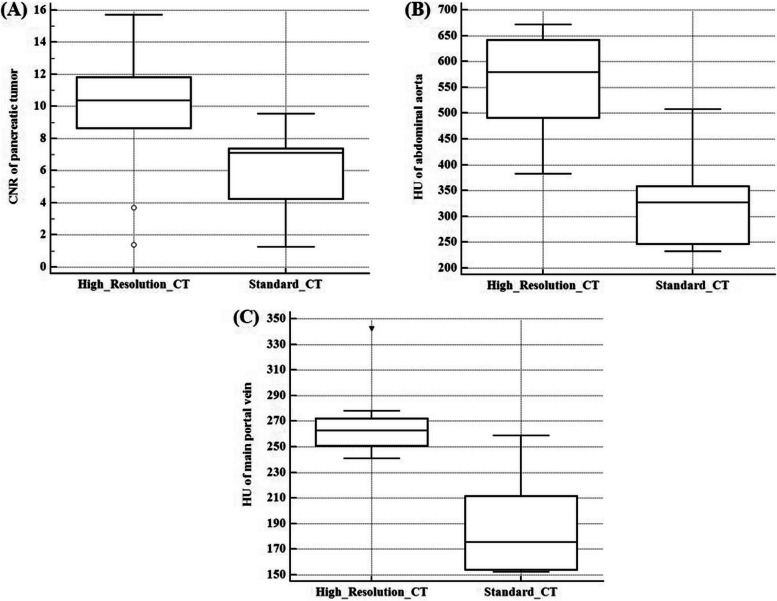
Results: A total of 69 patients (37 males and 32 females; median age, 66.5 years) were included in the study. The median CNR of PDAC was 10.4 in HR-CT, which was significantly higher than the 7.1 in the standard CT (P=0.006). Furthermore, HR-CT demonstrated notably higher median attenuation values for both the abdominal aorta (579.5 HU vs. 327.2 HU; P=0.002) and the MPV (263.0 HU vs. 175.6 HU; P=0.004) in comparison with standard CT. Following surgery, R0 resection was achieved in 51 patients. The pooled AUC for HR-CT in predicting R0 resection was 0.727, slightly exceeding the 0.699 of standard CT, albeit lacking a significant statistical distinction (P=0.128).
Conclusion: While HR pancreas CT using 80 kVp offered a notably greater degree of contrast enhancement in vessels and a higher CNR for PDAC compared to standard CT, its diagnostic performance in predicting R0 resection remained statistically comparable.
Keywords: High-resolution pancreas CT; Pancreatic ductal adenocarcinoma; Resectability assessment.
© 2023. The Author(s).
Conflict of interest statement
Jeong Min Lee: Grant from Bayer, Bracco, Canon, Central Medical Servis, Dongkuk Pharma, GE Healthcare, Guerbet, Philips Healthcare, Samsung Medison, Siemens Healthineers; Consulting fees from Sansumg medison; Honoraria from Bayer, Claripi, GE Healthcare, Guerbet, Philips Healthcare, Samsung Medison, Siemens Healthineers.
Dong Ho Lee: Research Grants from Canon Medical Systems.
Other authors declared no competing interests.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
