

Association of low muscle mass and obesity with increased all-cause and cardiovascular disease mortality in US adults
- PMID: 38111085
- PMCID: PMC10834318
- DOI: 10.1002/jcsm.13397
Association of low muscle mass and obesity with increased all-cause and cardiovascular disease mortality in US adults
Abstract
Background: Sarcopenic obesity, defined as the coexistence of low muscle mass and high adiposity, is associated with cardiovascular disease (CVD) and mortality. However, to what extent sarcopenia contributes to these risks independently or in conjunction with other cardiovascular risk factors remains unclear. This study aimed to investigate the association of low muscle mass, central obesity (COB), metabolic abnormalities, and their combinations with CVD and mortality risk.
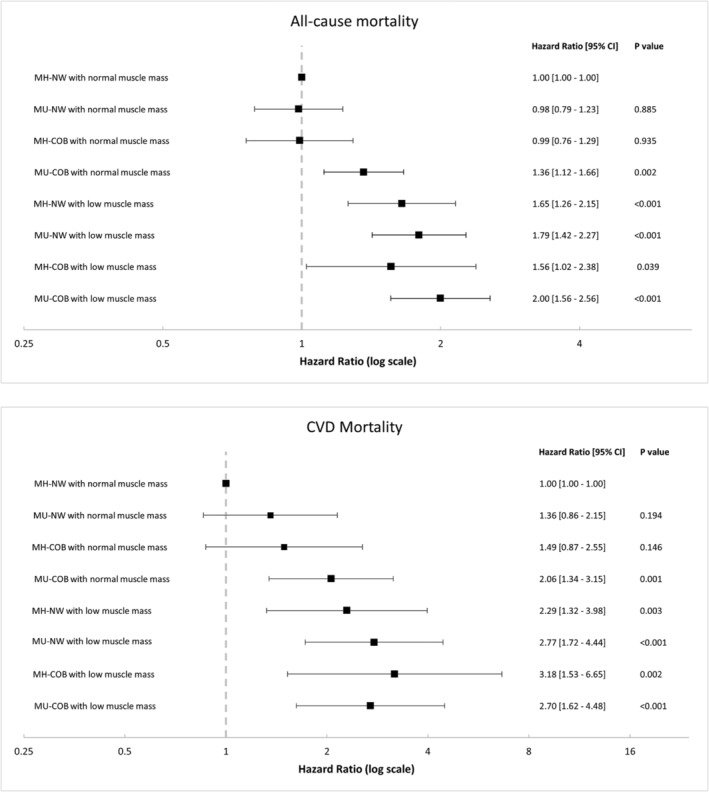
Methods: This cross-sectional analysis used data from the National Health and Nutrition Examination Survey 1999-2006 and 2011-2018. Participants aged >20 years and with reported whole-body dual X-ray absorptiometry data were included. Participants were divided into eight groups based on low muscle mass, metabolic abnormalities, and COB status.
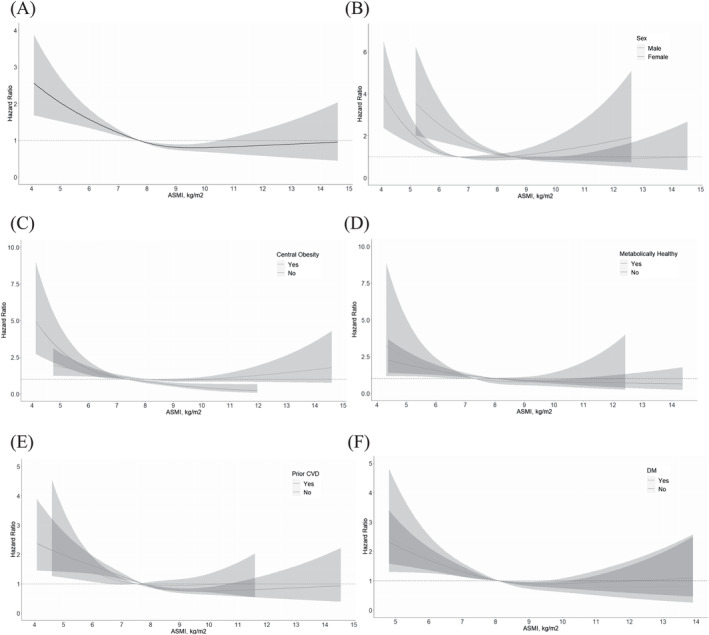
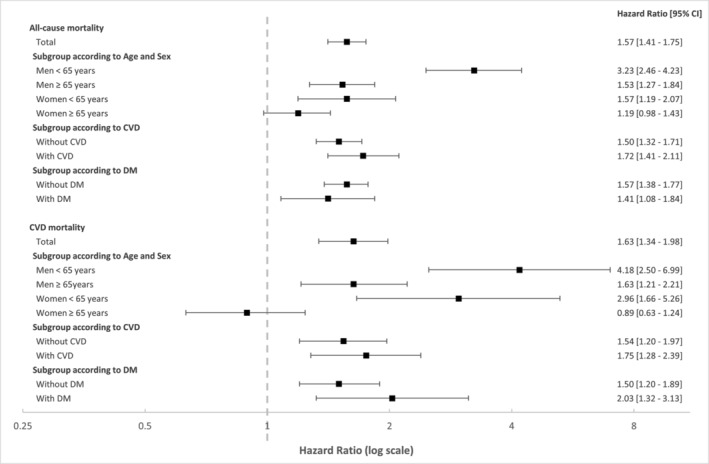
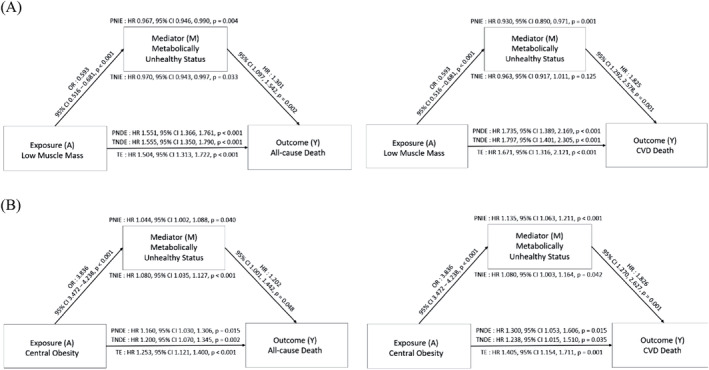
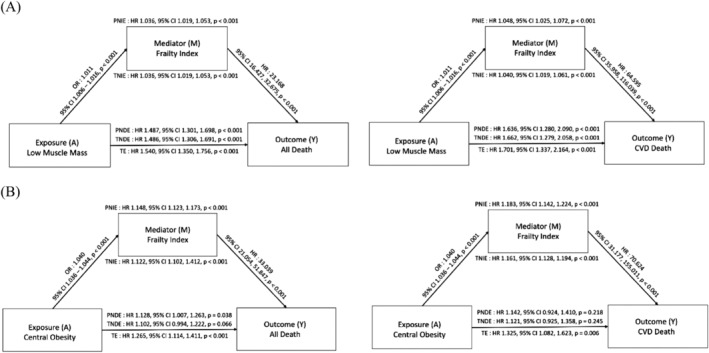
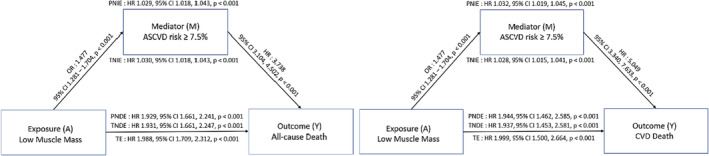
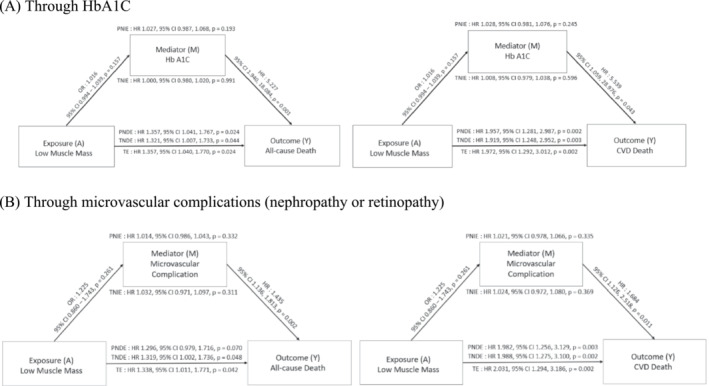
Results: The mean age of participants was 55 years, and 50.4% of participants were male. Low muscle mass was observed in 2472 (14.6%) out of 16 839 participants. Among the eight groups, the metabolically unhealthy COB group with low muscle mass had the highest hazard ratio (HR) for all-cause mortality (HR, 2.00; 95% CI, 1.56-2.56; P < 0.001), whereas the metabolically healthy COB group with low muscle mass had the highest HR for CVD mortality (HR, 3.18; 95% CI, 1.53-6.65; P = 0.001). The mediation analysis showed that low muscle mass directly increased the risk of both all-cause mortality (HR, 1.56; 95% CI, 1.35-1.79; P < 0.001) and CVD mortality (HR, 1.80; 95% CI, 1.40-2.31; P < 0.001). Additionally, subgroup analysis revealed that low muscle mass significantly increased the risk of all-cause and CVD mortality in participants without a prior CVD history and those with diabetes mellitus.
Conclusions: Low muscle mass is an independent risk factor for all-cause and CVD mortality, especially in individuals with metabolic abnormalities and COB.
Keywords: Cardiovascular disease; Central obesity; Metabolic syndrome; Sarcopenia.
© 2023 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
All the authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
