

Risk-benefit trade-offs and precision utilities in phase I-II clinical trials
- PMID: 38111231
- PMCID: PMC11132955
- DOI: 10.1177/17407745231214750
Risk-benefit trade-offs and precision utilities in phase I-II clinical trials
Abstract
Background: Identifying optimal doses in early-phase clinical trials is critically important. Therapies administered at doses that are either unsafe or biologically ineffective are unlikely to be successful in subsequent clinical trials or to obtain regulatory approval. Identifying appropriate doses for new agents is a complex process that involves balancing the risks and benefits of outcomes such as biological efficacy, toxicity, and patient quality of life.
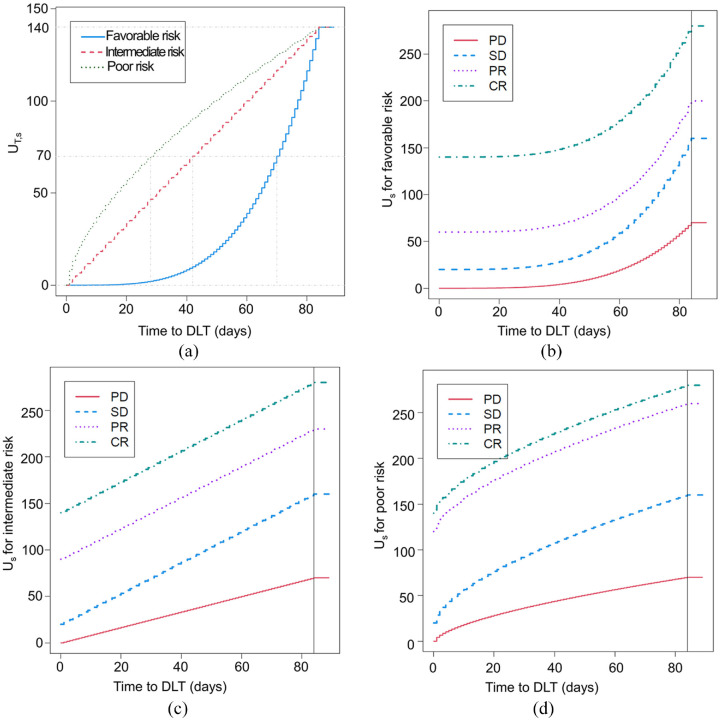
Purpose: While conventional phase I trials rely solely on toxicity to determine doses, phase I-II trials explicitly account for both efficacy and toxicity, which enables them to identify doses that provide the most favorable risk-benefit trade-offs. It is also important to account for patient covariates, since one-size-fits-all treatment decisions are likely to be suboptimal within subgroups determined by prognostic variables or biomarkers. Notably, the selection of estimands can influence our conclusions based on the prognostic subgroup studied. For example, assuming monotonicity of the probability of response, higher treatment doses may yield more pronounced efficacy in favorable prognosis compared to poor prognosis subgroups when the estimand is mean or median survival. Conversely, when the estimand is the 3-month survival probability, higher treatment doses produce more pronounced efficacy in poor prognosis compared to favorable prognosis subgroups.
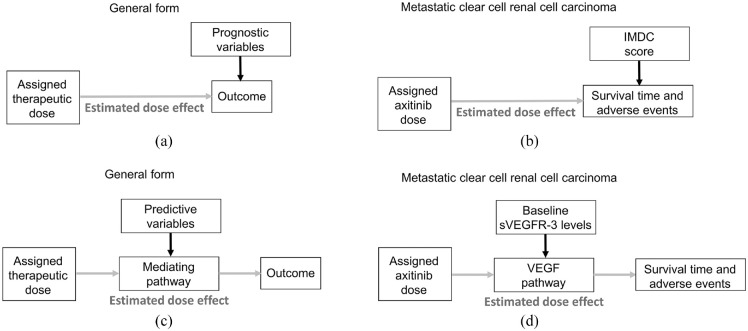
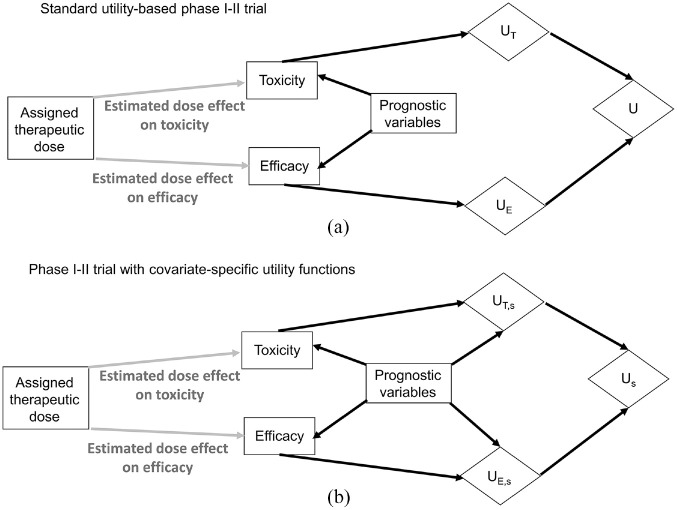
Methods and conclusions: Herein, we first describe why it is essential to consider clinical practice when designing a clinical trial and outline a stepwise process for doing this. We then review a precision phase I-II design based on utilities tailored to prognostic subgroups that characterize efficacy-toxicity risk-benefit trade-offs. The design chooses each patient's dose to optimize their expected utility and allows patients in different prognostic subgroups to have different optimal doses. We illustrate the design with a dose-finding trial of a new therapeutic agent for metastatic clear cell renal cell carcinoma.
Keywords: Covariate-specific utilities; personalized medicine; phase I-II trials; prognostic subgroups; risk–benefit trade-offs; utility functions.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.M. reports honoraria for scientific advisory board membership for Mirati Therapeutics, Bristol Myers Squibb, and Exelixis; consulting fees from Axiom Healthcare; non-branded educational programs supported by Exelixis and Pfizer; leadership or fiduciary roles as a Medical Steering Committee member for the Kidney Cancer Association and a Kidney Cancer Scientific Advisory Board member for KCCure; and research funding from Takeda, Bristol Myers Squibb, Mirati Therapeutics, and Gateway for Cancer Research.
Figures

References
-
- Hay M, Thomas DW, Craighead JL, et al.. Clinical development success rates for investigational drugs. Nat Biotechnol 2014; 32(1): 40–51. - PubMed
-
- Yuan Y, Nguyen HQ, Thall PF. Bayesian designs for phase I-II clinical trials. Boca Raton, FL: CRC Press, 2015.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
