

Considerations for hormonal therapy in migraine patients: a critical review of current practice
- PMID: 38112066
- PMCID: PMC10791067
- DOI: 10.1080/14737175.2023.2296610
Considerations for hormonal therapy in migraine patients: a critical review of current practice
Abstract
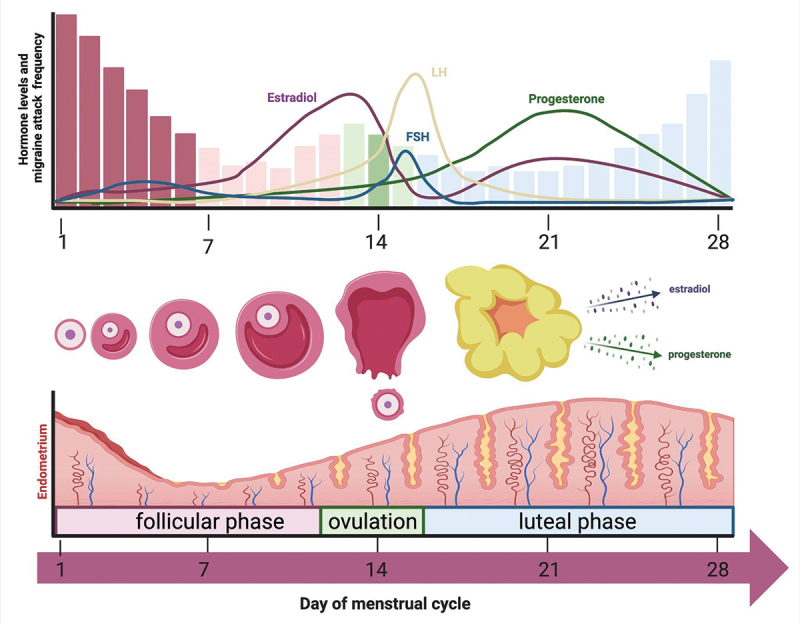
Introduction: Migraine, a neurovascular headache disorder, is a leading cause of disability worldwide. Within the multifaceted pathophysiology of migraine, hormonal fluctuations play an evident triggering and exacerbating role, pointing toward the need for identification and proper usage of both existing and new hormonal targets in migraine treatment.
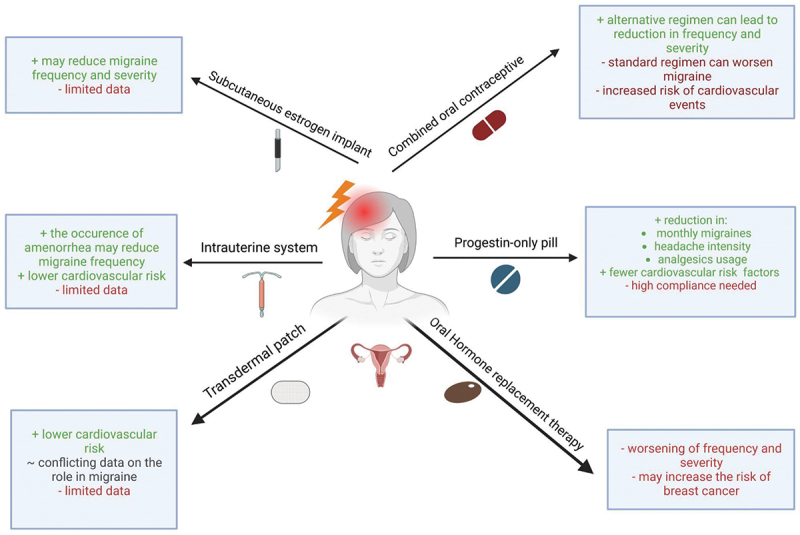
Areas covered: With a threefold higher incidence of migraine in women than in men, the authors delve into sex hormone-related events in migraine patients. A comprehensive overview is given of existing hormonal therapies, including oral contraceptives, intrauterine devices, transdermal and subcutaneous estradiol patches, gnRH-agonists, oral testosterone, and 5α reductase inhibitors. The authors discuss their effectiveness and risks, noting their suitability for different patient profiles. Next, novel evolving hormonal treatments, such as oxytocin and prolactin, are explored. Lastly, the authors cover hormonal conditions associated with migraine, such as polycystic ovary syndrome, endometriosis, and transgender persons receiving gender affirming hormone therapy, aiming to provide more personalized and effective solutions for migraine management.
Expert opinion: Rigorous research into both existing and new hormonal targets, as well as the underlying pathophysiology, is needed to support a tailored approach in migraine treatment, in an ongoing effort to alleviate the impact of migraine on individuals and society.
Keywords: Females; males; menopause; menstruation; migraine; pharmacology; sex hormones; treatment.
Conflict of interest statement
C Lampl has received fees as speaker or for participation to advisory boards from Allergan, Eli Lilly and Company, Novartis, Pfizer, and Teva. C Lampl is also the President of the European Headache Federation and Associated Editor of the Journal of Headache and Pain. A MaassenVanDenBrink has received research grants and/or consultation fees from Allergan, Amgen/Novartis, Eli Lilly and Company, Satsuma, Teva, and ATI. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
Similar articles
-
Sex hormones and headache.Rev Neurol (Paris). 2000;156 Suppl 4:4S30-41. Rev Neurol (Paris). 2000. PMID: 11139745 Review.
-
Sex and Gender Considerations in Episodic Migraine.Curr Pain Headache Rep. 2022 Jul;26(7):505-516. doi: 10.1007/s11916-022-01052-8. Epub 2022 Jun 9. Curr Pain Headache Rep. 2022. PMID: 35679008 Free PMC article. Review.
-
Sex hormones and headache.J Pain Symptom Manage. 1993 Feb;8(2):98-114. doi: 10.1016/0885-3924(93)90107-7. J Pain Symptom Manage. 1993. PMID: 8492007 Review.
-
Framing and Management of Migraines in Women: An Expert Opinion on Challenges, Current Approaches, and Future Multidisciplinary Perspectives.Healthcare (Basel). 2025 Jan 16;13(2):164. doi: 10.3390/healthcare13020164. Healthcare (Basel). 2025. PMID: 39857191 Free PMC article.
-
Hormone-related headache: pathophysiology and treatment.CNS Drugs. 2006;20(2):125-41. doi: 10.2165/00023210-200620020-00004. CNS Drugs. 2006. PMID: 16478288 Review.
Cited by
-
Sex difference in TRPM3 channel functioning in nociceptive and vascular systems: an emerging target for migraine therapy in females?J Headache Pain. 2025 Feb 24;26(1):40. doi: 10.1186/s10194-025-01966-9. J Headache Pain. 2025. PMID: 39994546 Free PMC article. Review.
-
Gender-specific inflammatory burden and headache risk in youth: a NHANES analysis.Head Face Med. 2024 Dec 5;20(1):71. doi: 10.1186/s13005-024-00475-5. Head Face Med. 2024. PMID: 39633488 Free PMC article.
-
Commentary: Improvement in diagnostic-therapeutic care pathways for women with migraine: an Italian Delphi panel.Front Neurol. 2024 Nov 20;15:1507261. doi: 10.3389/fneur.2024.1507261. eCollection 2024. Front Neurol. 2024. PMID: 39634775 Free PMC article. No abstract available.
-
Position paper of the expert panel of the Polish Society of Menopause and Andropause on the use of Oestrogel® in menopausal hormone therapy.Prz Menopauzalny. 2025 Jun;24(2):131-136. doi: 10.5114/pm.2025.152241. Epub 2025 Jun 23. Prz Menopauzalny. 2025. PMID: 40777875 Free PMC article. Review.
-
Sexual Dimorphism in Migraine. Focus on Mitochondria.Curr Pain Headache Rep. 2025 Jan 6;29(1):11. doi: 10.1007/s11916-024-01317-4. Curr Pain Headache Rep. 2025. PMID: 39760955 Review.
References
Publication types
LinkOut - more resources
Full Text Sources